Humeral Head Osteochondral Allograft Transplantation for a Contained Humeral Head Defect
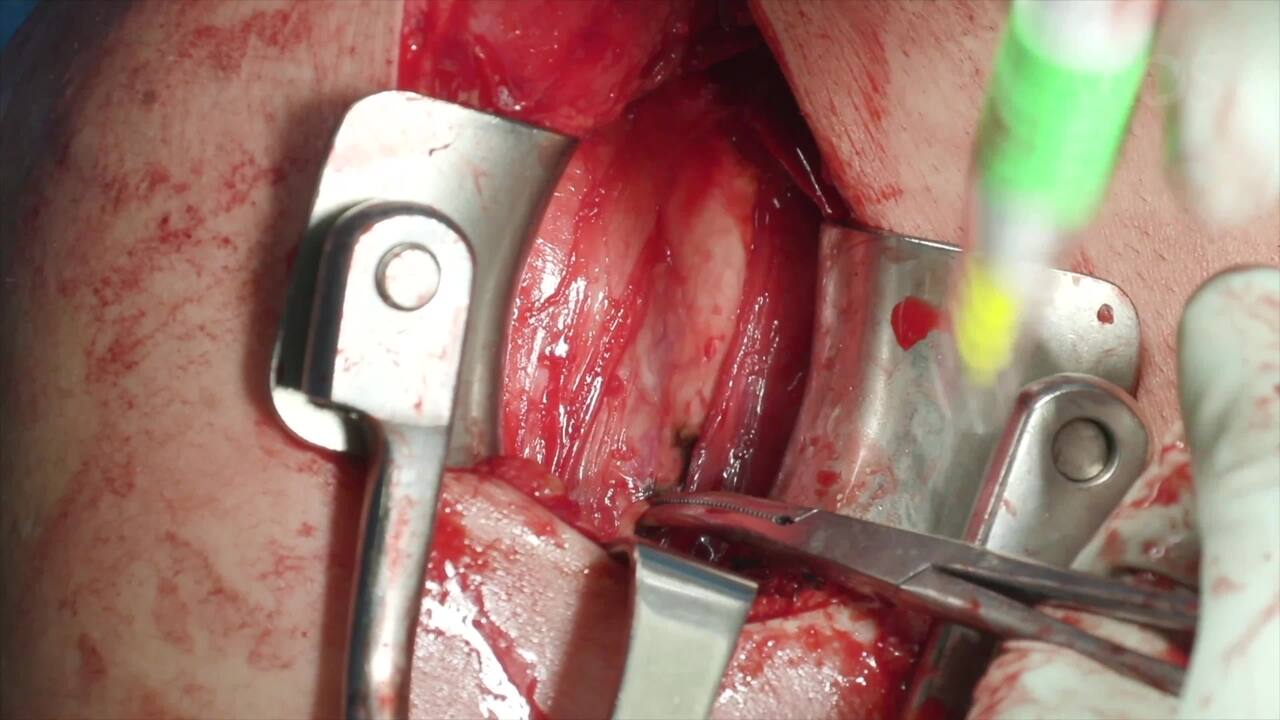
Background: Humeral head osteochondral lesions are less frequently encountered compared to locations such as the femoral condyles or talus, but have been reported in up to 17% of patients undergoing shoulder arthroscopy. Although they may be underdiagnosed and perhaps better tolerated than weight bearing joints like the knee or ankle, they can significantly affect shoulder function and cause pain. Various surgical treatment options exist and are dependent on both patient and lesional factors. Larger defects in younger, active patients are best addressed with autologous chondrocyte transplantation for isolated cartilage lesions or osteochondral allograft transplantation for lesions with subchondral bone involvement.Purpose: This video overview and case presentation demonstrates a humeral head osteochondral allograft transplantation for a contained humeral head defect in a young, active patient.Methods: The anatomy, classification, diagnosis, and treatment options for humeral head osteochondral defects are reviewed. The case of a 46-year-old male who underwent shoulder arthroscopy to address his biceps pathology, which demonstrated a unipolar, 4 mm2 posterosuperior humeral head osteochondral lesion, is presented. Postoperatively, the patient’s pain, limited range of motion (ROM), and mechanical symptoms failed to improve despite extensive physical therapy, anti-inflammatory use, and injections. After a thorough discussion of risks, benefits and prognosis, the patient elected to proceed with an open humeral head osteochondral allograft transplantation.Results: As anticipated, there was a 2 x 2 cm posterosuperior humeral head defect upon exposure of the glenohumeral joint via the deltopectoral approach. After the defect was appropriately prepared to a depth of 8 mm in all four quadrants, a 20 mm osteochondral plug, fashioned from a humeral head allograft, was press-fit into the recipient site. At 6 months post-operatively, the patient has ROM and strength equal to that of his contralateral shoulder. Advanced imaging demonstrates ongoing osseous integration of his graft with no perilesional arthritic progression.Conclusion: Often identified retroactively on imaging after arthroscopic diagnosis, humeral head osteochondral lesions can be the source of pain, ROM deficits, and mechanical symptoms for patients. Humeral head osteochondral allograft transplantation can effectively address larger lesions and restore glenohumeral concentricity with good short and mid-term ROM and clinical improvements.