Suture Recycling Techniques for Arthroscopic Shoulder Stabilization
Introduction: Many patients with shoulder instability require arthroscopic shoulder stabilization with labral repair. Typically, the torn labrum is reattached to the bony glenoid with the use of suture anchors. Multiple types of suture anchors are available, including standard suture anchors that require a knot to be tied and knotless suture anchors. A standard suture anchor can be loaded with two sutures for two points of soft-tissue fixation; however, the resulting tied knots have a relatively high profile in the joint space. A knotless suture anchor affords the mechanical benefit of eliminating knots in the joint space. One of the disadvantages of the knotless suture anchor is that it only can be loaded once, which limits the amount of soft tissue that can be re-approximated to the glenoid with the use of one anchor. Therefore, to achieve more than one point of fixation, multiple knotless suture anchors must be inserted into the glenoid when used in the traditional manner. Iatrogenic glenoid fracture is associated with the use of several anchors implanted in the glenoid rim. Regardless of the type of suture anchor used, a simple suture pass leaves suture in the joint space, which is another potential mechanical irritant. The novel technique described in this video recycles remaining suture limbs from knotless anchors for a second vertical mattress pass through soft tissue, providing two points of fixation per anchor. Using this suture recycling technique, the amount of suture in the joint space, the number of knots tied, and the number of anchors placed are reduced while increasing soft-tissue fixation.
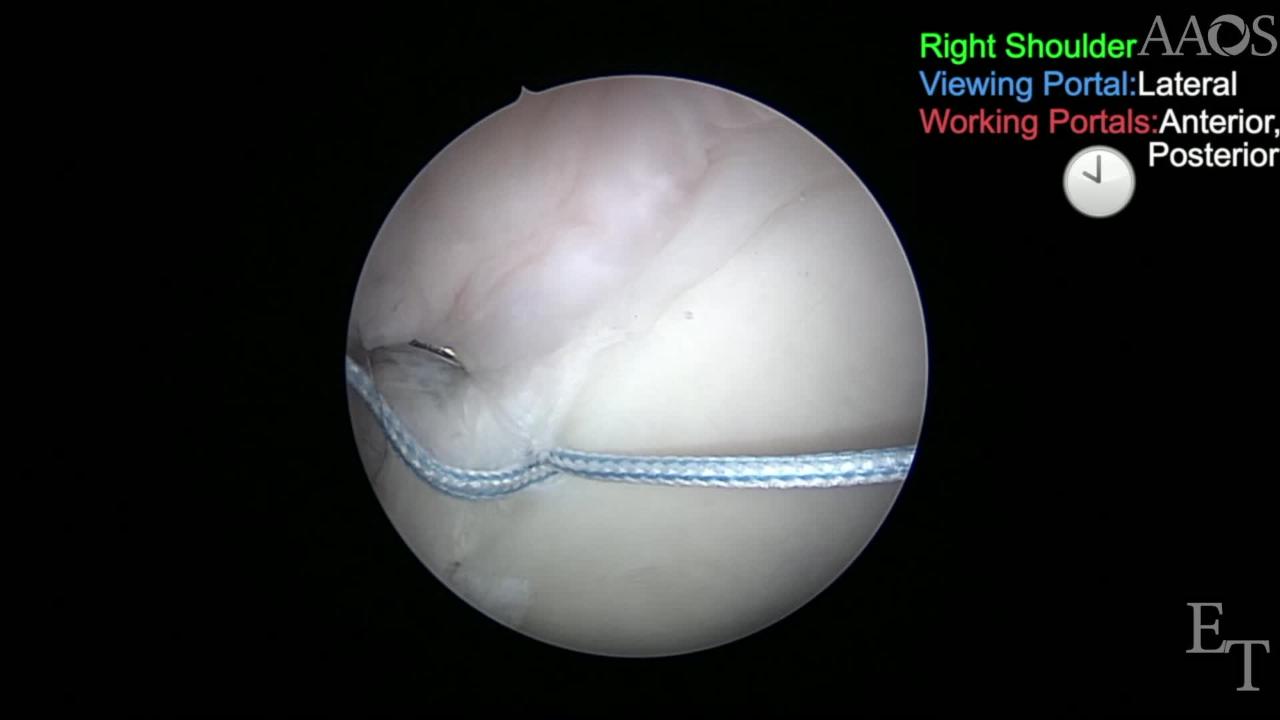
Procedure: The patient is placed in the beach-chair position on the surgical table. Arthroscopy of the shoulder is performed using four portals (anterior, posterior, posteroinferior, and lateral). Portals are made lateral with the use of a No. 11 scalpel blade that is taken down through the the skin and subcutaneous tissues. Each portal is then dilated with the use of a blunt obturator and cannula. Each portal, with the exception of the posterior portal, is made under direct arthroscopic visualization after localization with a spinal needle. The patulous glenohumeral labroligamentous complex is tightened to the glenoid with the use of suture anchors. A knotless suture anchor is inserted at the 10 o'clock position. The anchor is loaded with No. 2 nonresorbable suture. The labrum is plicated with the superior glenohumeral ligament via a vertical mattress recycling technique with knotless anchors. A suture passer is used to pass each suture around the glenohumeral labroligamentous complex in a vertical mattress fashion. The arthroscopic knotless anchor technique is used to perform the capsulorrhaphy. The residual suture limbs are then recycled for a second vertical mattress pass around the labrum and the superior glenohumeral labroligamentous complex for additional capsulorrhaphy. An arthroscopic knot tying technique is used to secure each knot after the second pass.