Anterolateral Ligament Repair via Augmentation
2019 HONORABLE MENTION
Anterior cruciate ligament (ACL) rupture is a common sports-related injury. ACL reconstruction has long been the preferred treatment option for the surgical management of ACL ruptures. Recent surgical and imaging studies have demonstrated anterolateral ligament (ALL) injury in approximately 90% of patients with an ACL tear. Various extra-articular surgical techniques have been proposed to better restore rotational stability of the knee. However, concern exists that lateral extra-articular reconstruction is nonanatomic and may overconstrain the joint because of altered biomechanics. Surgical repair of the ALL may be considered in patients with an acute ACL tear to achieve anatomic reconstruction. Furthermore, the addition of an augmentation with increased mechanical properties may afford a load sharing, and thus protective, effect for the repair during healing.
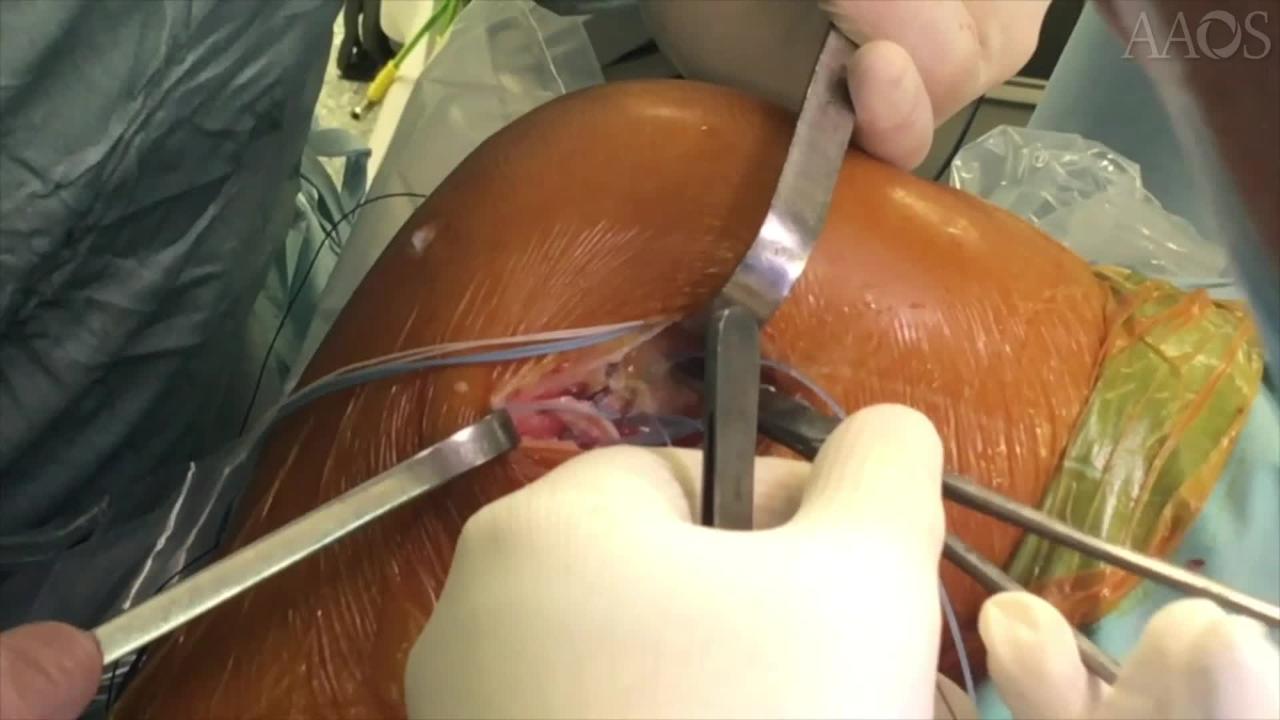
This video demonstrates ALL repair via augmentation. The study included three patients who underwent reconstruction for the management of an acute ACL tear between January 2017 and May 2017. Inclusion criteria were an acute ACL tear, severe rotational instability (pivot-shift =3), and surgical management within 10 days postinjury. With the knee in 90° degrees of flexion, a 4- to 5-cm hockey-stick incision is made on the lateral aspect of the knee from the lateral femoral condyle to the Gerdy tubercle. The peroneal nerve is moved distal to the surgical field to prevent injury during the procedure. After dissection of the skin and subcutaneous tissue, the iliotibial band is visualized and incised along its fibers to expose the anterolateral capsule. The lesions of the ALL and capsule are visualized and recorded. The injury is directly repaired based on the type of lesion. A 2.4-mm Kirschner wire is placed at the anatomic tibial insertion of the ALL, halfway between the Gerdy tubercle and the fibular head. This point is approximately 22 mm from the center of the Gerdy tubercle and 11 mm below the joint line. The lateral collateral ligament and the popliteus tendon are visualized and protected. A second 2.4-mm Kirschner wire is inserted at the femoral insertion of the ALL, just proximal and posterior to the lateral femoral epicondyle. Any interference with the femoral ACL tunnel should be avoided. Tension is assessed during range of motion between 0° and 90° of flexion. The goal is to attain a bundle that is tight in extension and slack in flexion, which reproduces the function of the ALL. A bone socket that is 20 mm in depth and 4.5 mm in diameter is drilled on tibial side. A No. 2 tape suture is loaded on a 4.75-mm knotless anchor and fixed on the tibial side underneath the iliotibial tract. With a free needle, the two sutures from the anchor and the two tapes loaded on the anchor are used to repair the ALL and capsule on the tibial insertion. A bone socket that is 20 mm in depth and 4.5 mm in diameter is drilled on the femoral side. The tape from the previously placed tibial anchor is loaded on a second 4.75-mm knotless anchor. The knee is placed in full extension, and the tape is fixed on the femoral side using manual tension. The final construct consists of an anatomic ALL repair with a tape augmentation fixed on the tibial and femoral anatomic insertions. The iliotibial tract is closed with No. 0 suture, and the skin incision is closed in a standard fashion. Of the three patients, two were men and 1 was a woman (mean age, 19.1 years). The mean follow up was 12 months. In all the patients, full range of motion was attained after 30 days.
The role of secondary rotatory restraints at the lateral aspect of the knee has been clearly shown in the literature. A number of lateral extra-articular procedures have been proposed to take advantage of the long lever arm, which acts as a lateral tenodesis. In a recent clinical study, ALL reconstruction in combination with ACL reconstruction using a hamstring graft resulted in good clinical outcomes and a decreased failure rate at a follow-up of 2 years. Techniques have shifted from nonanatomic procedures to procedures attempting to reproduce anatomy. Anatomic ALL reconstruction techniques using soft-tissue grafts, such as the gracilis tendon and the fascia lata, have been proposed. However, acute repair rather than reconstruction of this ligamentous structure may be a treatment option to restore normal anatomy. The addition of an augmentation that acts as a seatbelt support, ensuring anatomic length of the ligament during healing, has been proposed. The ALL is an important secondary stabilizer of the ACL, controlling rotational stability of the knee and the pivot-shift phenomenon. Repair of the ALL via augmentation may allow for faster rehabilitation, protecting the graft during healing.