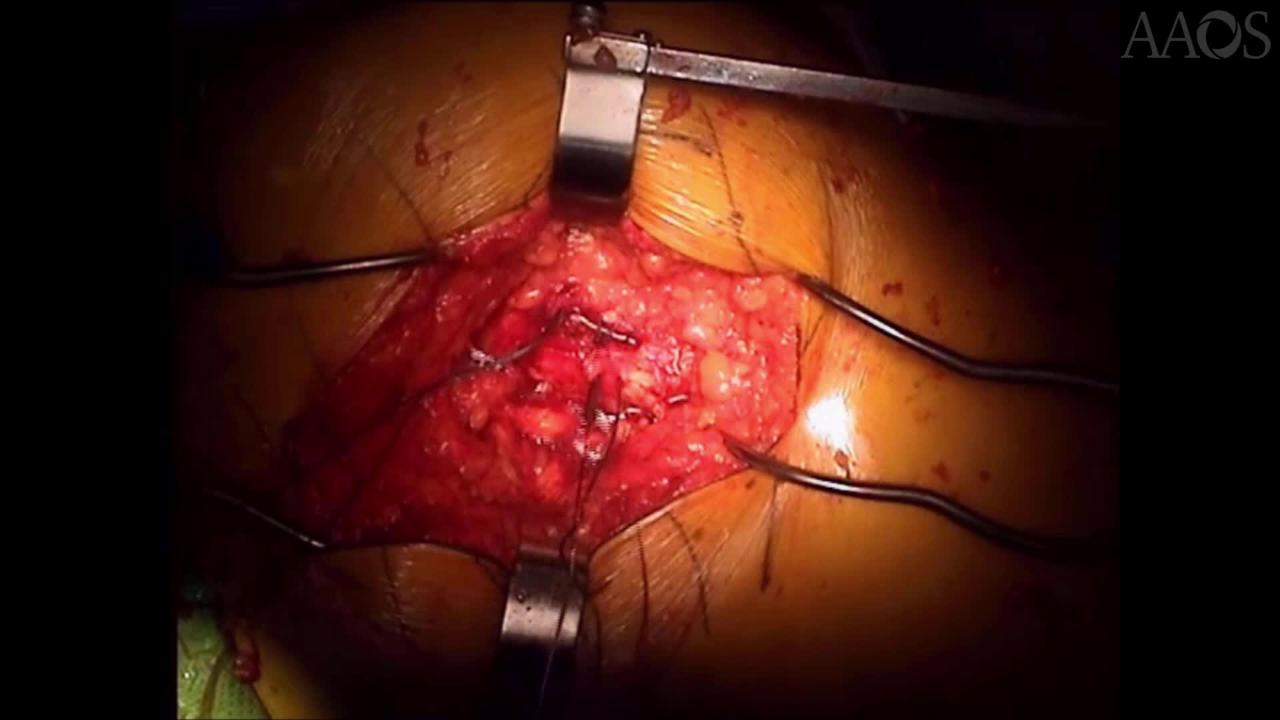
Open Tendon Repair Into a Bone Trough for Management of Hip Abductor Tendon Avulsion
Hip abductor tendon tears are likened to rotator cuff tears of the hip, causing progressive lateral hip pain, weakness, and limp. This video compares the short-term clinical outcomes of open abductor tendon repair via decortication and suture fixation (DSF) with those of open abductor tendon repair into a bone trough (BT). In addition, the video examines the results of repair in small tears and large tears.
Forty-two consecutive hip abductor tendon repairs performed between January 2009 and December 2017 were retrospectively reviewed. Small tears were defined as partial-thickness tears, longitudinal tears (repaired side-by-side), and isolated gluteus minimus tears (repaired via tenodesis to the gluteus medius). Large tears were defined as full-thickness avulsion of 33% to 100% of the gluteus medius insertion, with or without gluteus minimus tear. DSF was used for the management of 15 tears, and BT was used for the management of 10 tears. Preoperative and postoperative pain, the ability to perform single leg stance, hip abduction, clinical strength (0 to 5 scale), and Trendelenburg lurch were examined. Standard statistical analyses were used, with a type I error being a = 0.05. Of the 42 abductor tendon repairs identified, 5 were excluded, leaving 25 large tear repairs and 12 small tear repairs (mean follow up, 21 months). Comparing the outcomes of large tear repair, repair into a BT was associated with a lower failure rate (0 versus 6 [40%], respectively), greater reduction in pain at 1 year postoperatively (change in visual analog pain score, -5.70 ± 0.97 versus -2.73 ± 0.69, respectively), better ability to perform single leg stance (90% versus 47%, respectively), and better hip abduction (100% versus 73%, respectively) than repair via DSF. Clinical strength trended higher for repairs into a BT but did not reach statistical significance. Comparing the outcomes of large tear repair with those of small tear repair, small tear repair was associated with lower visual analog scale pain scores and increased clinical strength preoperatively and 1 year postoperatively. Small tear repair was associated with better ability to perform single leg stance (100% versus 64%, respectively) and better hip abduction (100% versus 78%, respectively) compared with large tear repair. Finally, large tear repair was associated with a statistically higher residual Trendelenburg lurch compared with small tear repair (56% versus 0, respectively). The outcomes of abduction tendon repair are better in patients with a small tear than patients with a large avulsion, which is an important finding compared with that reported in the literature on abductor tendon repair. Abductor tendon repair of large avulsions into a BT resulted in substantially improved surgical results.