Staged Reconstruction of Multiligamentous Knee Injuries
Multiligamentous knee injuries are devastating injuries that may lead to chronic instability, nerve damage, and early-onset osteoarthritis. In general, multiligamentous knee injuries are classified based on the number of torn ligaments, which helps guide surgical planning and management. Recent data have shown that early surgical management (<3 weeks postinjury) leads to improved patient outcomes. However, debate exists with regard to whether acute surgical management should consist of repair, repair with augmentation, or reconstruction of the posterolateral corner.
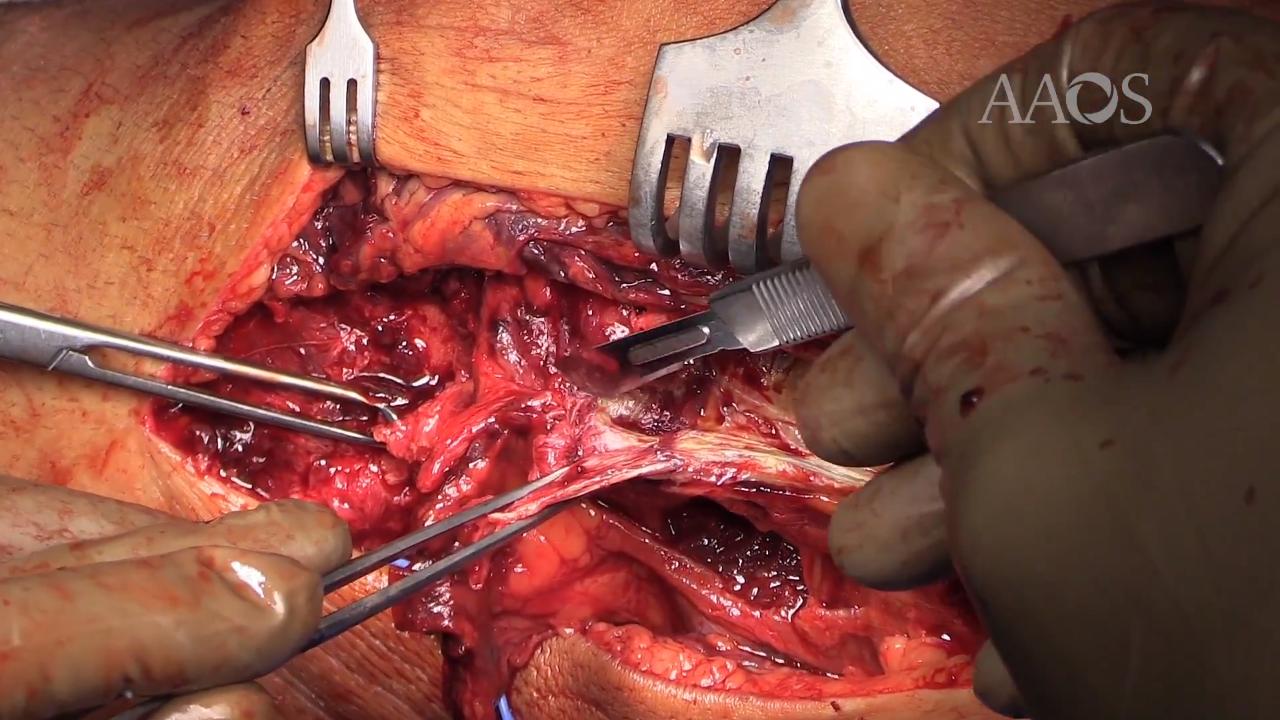
This video demonstrates the technique for staged management of a multiligamentous knee injury. The video discusses the case presentation of a young, active 36-year-old man who sustained a knee injury when playing basketball and requires surgery for the management of a torn anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), and posterolateral corner. The posterolateral corner is managed acutely (<3 weeks postinjury) via repair and augmentation with the use of an allograft. After appropriate postoperative physical therapy and improvement in range of motion (12 weeks postoperatively), ACL and PCL reconstruction are performed.
This video discusses the presentation and examination of multiligamentous knee injuries and decision-making strategies for management. Preoperative MRIs are provided and discussed. Outcome data on posterolateral corner repair in the acute setting and return to sport after multiligamentous injury are described.
Postoperative management is specifically discussed because it is vital in the staged management of this patient. A strict non–weight-bearing protocol for 6 weeks and limited range of motion in a hinged knee brace that is locked in extension are essential in the initial postoperative period. Patient expectations and goals must be discussed preoperatively to ensure postoperative compliance to allow for soft-tissue healing and graft uptake. Passive range of motion was initiated at 3 weeks postoperatively, with a goal of full range of motion by 12 weeks postoperatively. The patient should remain non–weight bearing for a total of 6 weeks postoperatively, with weight bearing gradually increased to full weight bearing by 10 weeks postoperatively.
Staged management of multiligamentous knee injuries is a good option for patients undergoing early surgical management. Early repair of the posterolateral structures and staged ACL/PCL reconstruction may afford good outcomes and improved stability.