Severe Varus Knee
Adequate soft-tissue release is essential to restore the normal mechanical axis is a patient with a severe varus knee. This method for medial release avoids over-release and is reproducible and easy. This method only involves needle puncturing of the soft tissue and does not require release of the superficial medial collateral ligament and the pes anserinus from the attachment. This method is selective and sequential according to the degree and site of imbalance. The patient in this video had 17° of genu varum.
1. The incision is started 3 cm above the patella, and the knee joint is exposed via an anteromedial approach.
2. After a medial parapatellar arthrotomy, the deep medial collateral ligament and the adjacent posteromedial capsules are released subperiosteally until the lower margin of the osteophytes are exposed.
3. The femoral canal is opened with the use of a 9.5-mm intramedullary drill and an intramedullary guide aimed at the mechanical axis.
4. The distal femur is resected with the use of an oscillating saw.
5. The anterior and posterior cruciate ligaments are sacrificed.
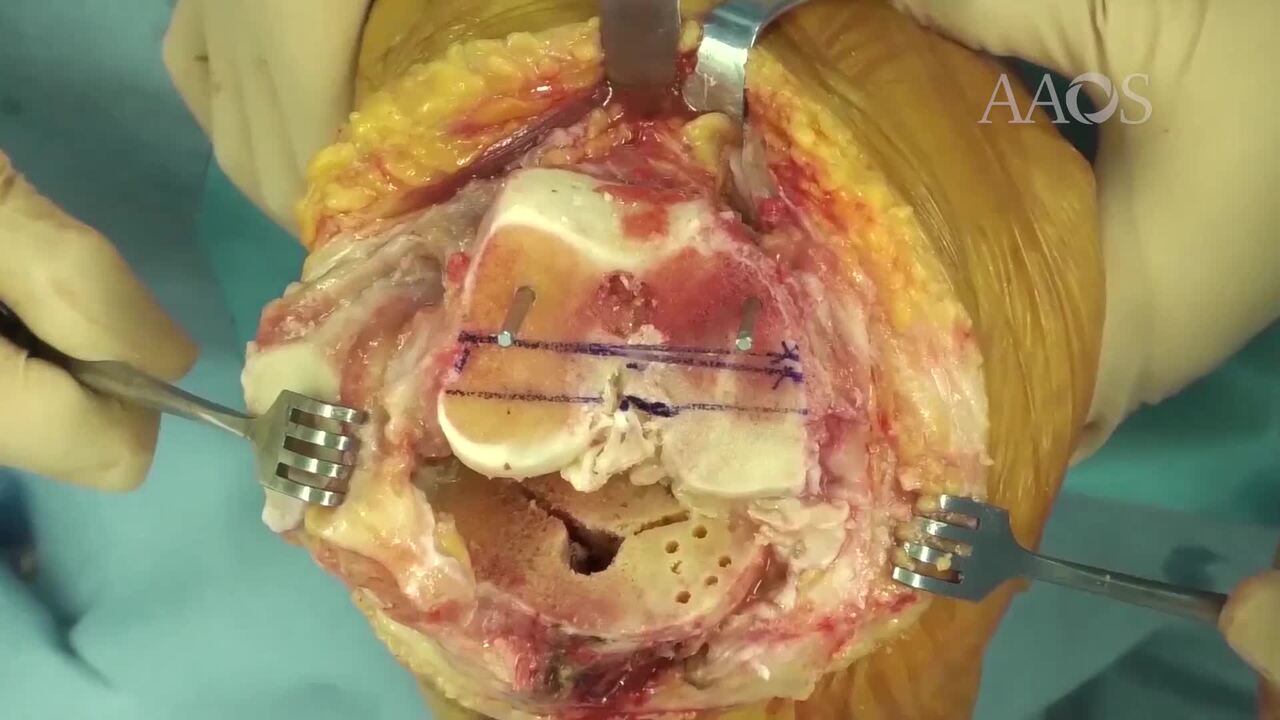
6. The proximal tibia is resected with the use of an extramedullary guide and the oscillating saw.
7. After tibial component sizing, residual bone and osteophytes are removed.
8. Approximately 3° of external rotation is applied relative to the posterior condylar axis. If necessary, rotation is adjusted according to the transepicondylar axis.
9. After femoral component sizing, anterior flange, posterior condyle, and chamfer cutting are sequentially performed.
10. The appropriately sized femoral trial is applied.
11. Posterior osteophytes are removed with the use of a curved osteotome, and remaining osteophytes are assessed at the gap between the medial collateral ligament and the medial end of the distal cut surface.
12. The medial and lateral gaps are measured in full extension and in 90° of flexion with the use of a tensor device.
13. In this patient, the medial gap was 22 mm, which was smaller compared with the lateral gap.
14. Using a spinal needle, the superficial medial collateral ligament is punctured three times on the anterior side and three times on the posterior side.
15. The medial flexion gap is gently and gradually spread with the use of a spreader.
16. After needle puncturing, the medial and lateral gaps are balanced.
17. The appropriate articular insert trial is placed onto the tibial trial.
18. Range of motion, full extension, and laxity are assessed.
19. A rongeur is used to remove osteophytes and reduce the patella to its true size.
20. The final component is applied with the use of cement.
21. Fixation of the components is assessed.