Patellar Tendon Reconstruction Using Semitendinosus Autograft of Patellar Tendon Rupture After Bone-Patellar Tendon-Bone Anterior Cruciate Ligament Reconstruction
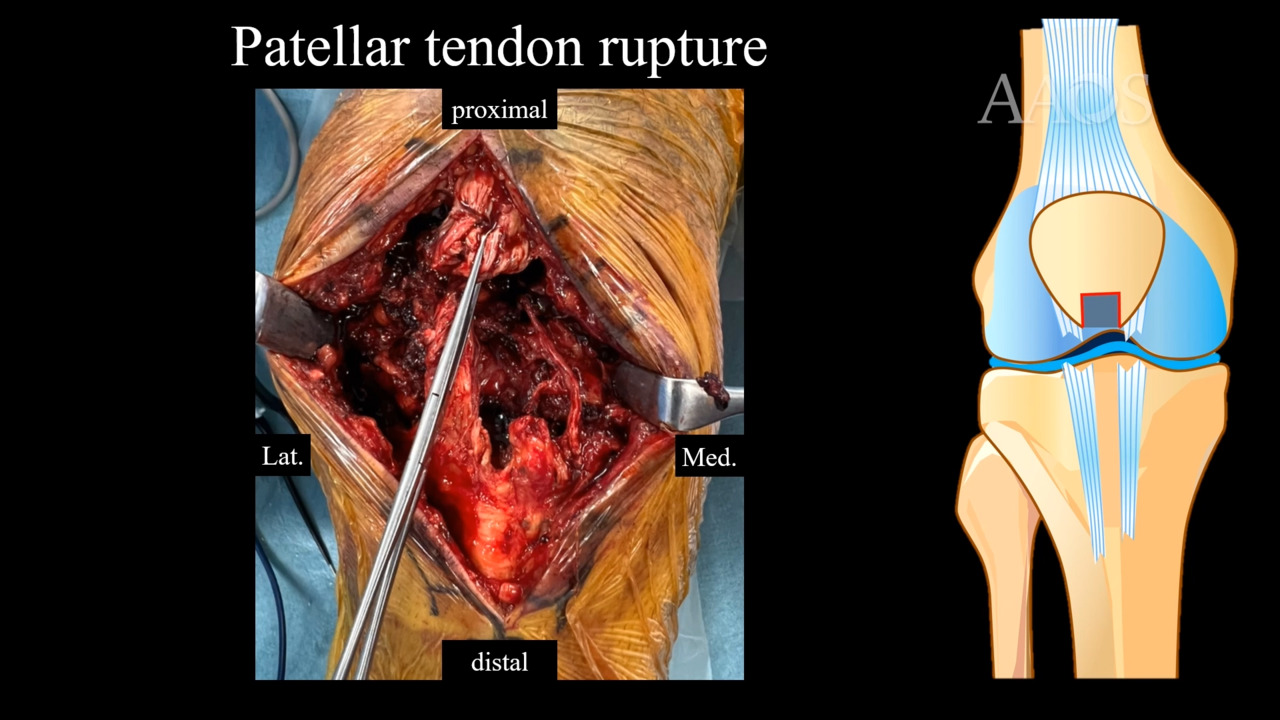
Patellar tendon rupture after bone-patellar tendon-bone (BPTB) anterior cruciate ligament reconstruction is a rare but known complication. If the extensor mechanism fails after BPTB harvest, it commonly results in a patellar fracture. The rate of patellar tendon rupture has been reported to be approximately 0.25%, whereas patellar fractures are observed at a rate of 1.3%. Patellar tendon rupture can occur in the early postoperative period, usually attributed to slip and fall–type injuries, or may be a late manifestation resulting from forced eccentric contraction of a flexed knee. Various treatment options for patellar tendon rupture have been reported. Bone-tendon-bone autografts with strong fixation require the graft to be harvested from a healthy knee. Shelbourne et al reported that function is not affected, whereas Temponi et al reported that function does not return to preinjury levels. Hesitation to perform another BPTB harvest for a rupture exists after BPTB harvest. In proximal and distal ruptures, the tendon is brought back to its anatomic position and secured to the inferior pole of the patella or the tibial tuberosity and the medial and lateral retinacular tears are repaired. Midsubstance ruptures are repaired via sutures placed in proximal and distal bundles and secured through parallel vertical holes drilled in the patella, with a transverse hole drilled in the tibial tuberosity. However, after BPTB harvest, repair alone is not strong enough, and the risk of re-breakage is high. Therefore, the authors of this video perform augmentation with the use of hamstring tendon, using a transosseous tunnel at the tibial tubercle to preserve the distal attachment of the hamstring tendon while augmenting. The case presentation of a 35-year-old man who underwent left anterior cruciate ligament reconstruction using the central one-third of the BPTB autograft approximately 20 years ago is reviewed. The injuries were the result of falls while ascending stairs. Radiographs are shown. The lateral radiograph demonstrates patellar elevation on the affected side compared with the healthy side. CT scans show the central one-third of the patella was harvested and missing. MRIs show patellar tendon continuity was disrupted. A midline incision was made over the patella down to the tibial tubercle, incorporating the incision from the initial BPTB graft harvest. The patellar tendon had ruptured in the distal substance, leaving it attached to the tibia on the medial side. The lateral side had a substantial amount of tendon still attached to the patella. After the scar tissue was cleared and the patellar tendon was clearly identified, a separate medial incision was made to harvest the semitendinosus tendon with the use of an open-ended tendon stripper, preserving the distal attachment to the tibia. The harvested tendon was delivered into the central wound under soft tissue. After the harvested tendon was stripped of muscle tissue, a 4.0-mm drill hole was placed through the tibial tubercle below the attachment of the patellar tendon. The harvested tendon was then brought through the drill hole from medial to lateral and was incorporated into the proximal tendon along the inferior border of the patella. Based on the healthy knee, patellar tendon length was determined to be 50 mm. After the semitendinosus was weaved through the proximal tendon stump, it was placed in tension until the preinjury length of 50 mm was reestablished. The semitendinosus graft was then secured to the medial aspect of the tibia with the use of a 4.75-mm biocomposite anchor. Two interrupted No. 2 FiberWire sutures (Arthrex) were then placed at the proximal tendon stump. Finally, the patellar tendon was repaired with FiberWire and augmentation with semitendinosus through the bony foramen and FiberTape (Arthrex). Postoperative radiographs demonstrated resolution of patellar elevation. The patient's leg was placed in a brace locked in extension for 2 weeks until the wound had fully healed. At that point, the patient progressed to range of motion as tolerated. Return to sports activity was allowed in stages according to the recovery of muscle strength and the stability of movements on the affected side. Physical examination findings at 3 weeks postoperatively included no extension lag and good range of motion. Patellar tendon rupture after anterior cruciate ligament reconstruction with BPTB may be a devastating complication. This video demonstrates a successful technique for patellar tendon reconstruction with the use of semitendinosus autograft while maintaining the native attachment of the tendon on the anteromedial tibia.