Zone 1 Flexor Tendon Repair
Objectives
The objective of this video is to demonstrate zone 1 flexor tendon repair with the use of two transosseous tunnels through an incision of the tip of the distal phalanx.
Indications
An indication is retraction of the flexor digitorum profundus with inability to flex at the distal interphalangeal joint.
Contraindications
A contraindication is flexor digitorum profundus retraction into the palm for more than 6 to 8 weeks.
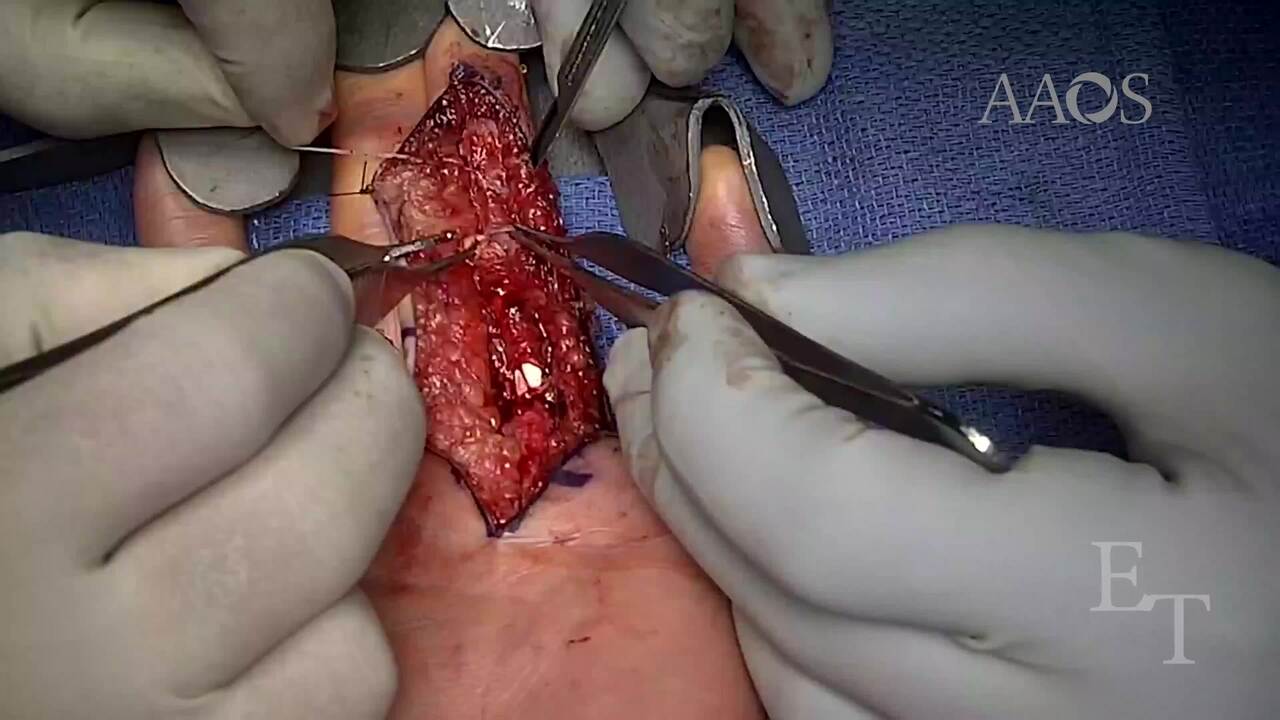
Surgical Technique
This video demonstrates zone 1 flexor tendon repair with the use of two transosseous tunnels through an incision of the tip of distal phalanx at which the suture will be passed. A mid-lateral incision is made from the distal interphalangeal joint flexion crease to the metacarpophalangeal joint flexion crease. Two additional oblique incisions are made on the distal ends to create a volar flap. Dissection is carried out through the soft tissues, and care is taken to identify and protect the neurovascular bundle, especially the ulnar digital bundle. The A2 and A4 pulleys are identified and loosened to allow for later passage of the flexor digitorum profundus tendon. A 3-0 FiberWire (Arthrex) suture is used in a running, locking fashion on the flexor digitorum profundus tendon. A nitinol suture passing wire is then passed distal to proximal to retrieve the suture limbs and retracted back out distally through the A2 pulley. This is repeated through the A4 pulley. If necessary, the fibroosseous sheath can be vented at the A4 pulley. Next, the transosseous tunnels are prepared by creating a horizontal incision at the distal phalanx followed by subperiosteal dissection at the dorsal proximal portion of the distal phalanx. A Kirschner wire is used to mark the insertion site for the flexor digitorum profundus on fluoroscopy followed by a 2-0 drill. A 0.45-mm Kirschner wire is passed from the distal phalanx, using two oblique passes, to allow for an adequate bone tunnel. A proper connection is then established between the transosseous tunnels and the flexor digitorum profundus insertion site. A nitinol suture passing wire is passed through the flexor digitorum profundus insertion site with the use of a passing stitch. The passing stitch is then used to retrieve one of the two limbs of the 3-0 FiberWire to be passed through the distal end of the transosseous tunnels. This is repeated within the other transosseous tunnel. A total of six knots are used to facilitate fixation of the FiberWire to the bone-tendon interface.
Postoperative Management
Immediately postoperatively, patient's arm is placed in a dorsal blocking splint with the wrist and metacarpophalangeal joint in flexion with the interphalangeal joint in extension. At 2 weeks postoperatively, the patient begins a modified Duran protocol with occupational therapy, and the dorsal blocking splint is removed. At 6 weeks postoperatively, the patient begins full active range of motion and strengthening.