Use of Augmented Reality Surgical Navigation Reduces Intraoperative Fluoroscopic Imaging in Anterior Total Hip Arthroplasty With Equivalent Accuracy for Component Positioning
Introduction
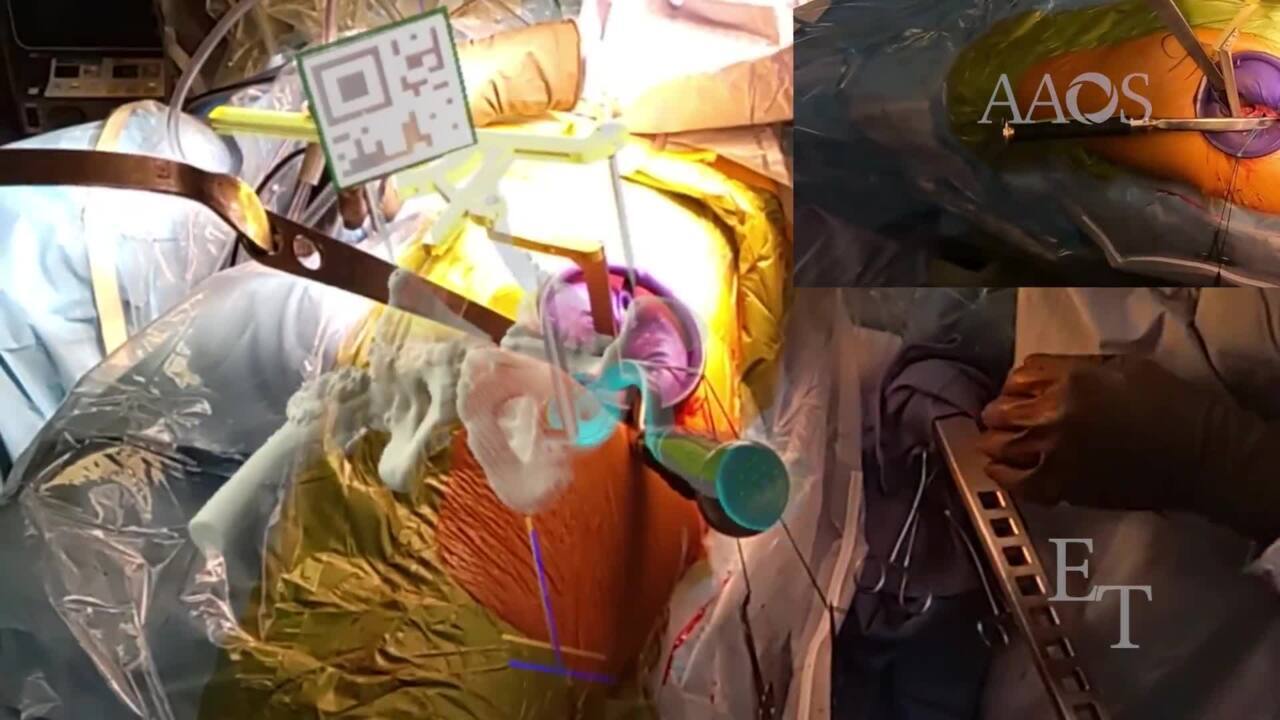
Acetabular component malpositioning is a major risk factor for determining the likelihood of revision after primary total hip arthroplasty (THA). Computer-assisted surgical navigation was designed to reduce the rate of acetabular component malpositioning; however, these technologies may be challenging to adopt. The goal of this video is to demonstrate a technique for intraoperative augmented reality surgical navigation for direct anterior total hip arthroplasty.
Methods
The video retrospectively reviews 30 hips managed via primary direct anterior THA performed with the use of an intraoperative augmented reality surgical navigation system. These hips were compared with 30 hips managed via primary direct anterior THA performed with the use of fluoroscopic assistance during the same time. An inclination of 42° and an anteversion of 25° were planned for all the hips. Demographics between the cohorts were similar.
Results
Patients who underwent THA with the use of an augmented reality surgical navigation system had decreased intraoperative radiation exposure (P = 0.004) and radiation time (P < 0.001). No differences in surgical time (P = 1.0), the use of cables (P = 1.0), estimated blood loss (P = 0.6), intraoperative complications (P = 1.0), or revision surgery (P = 1.0) were reported between the cohorts. The mean difference in radiographic inclination from the preoperative plan was -0.7° in the augmented reality group (range, -9.4° to 6.7°) and -1.3° in the manual group (range, -7.9° to 7.9°). The mean difference in radiographic anteversion from the preoperative plan was 0.0° in the augmented reality group (range, -12.2° to 7.0°) and -1.3° in the manual group (range, -12.8° to 17.1°). Most of the patients were within 5° of planned inclination and/or anteversion; this was similar between the augmented reality and manual cohorts (P = 0.7 and P = 0.4, respectively).
Conclusion
Augmented reality surgical navigation in primary direct anterior THA results in outcomes similar to those of manual THA with the use of intraoperative fluoroscopic assistance, including outcomes related to radiographic anteversion and inclination, surgical time, estimated blood loss, and revision surgery; however, augmented reality surgical navigation is associated with decreased intraoperative fluoroscopic radiation exposure and radiation time.
Additional research is necessary to evaluate the accuracy of acetabular component positioning and complications.