An Isolated Midsubstance Anterior Cruciate Ligament Tear Repaired With the Bridge-Enhanced Anterior Cruciate Ligament Repair System
Background
Anterior cruciate ligament (ACL) repair, although widely abandoned because of historically high failure rates, recently regained interest given the development of the bridge-enhanced anterior cruciate ligament repair (BEAR) implant, which is a novel arthroscopic technique that involves the use of a resorbable protein-based implant combined with autologous blood to primarily repair a midsubstance ACL tear. This video presents a step-by-step surgical method for management of an isolated midsubstance ACL tear via the BEAR implant.
Indications
The BEAR implant is indicated in skeletally mature patients aged 14 years or older who have a complete rupture of the ACL that is confirmed on MRI. The complete ACL tear must have an attached stump to the tibia.
Technique
Description
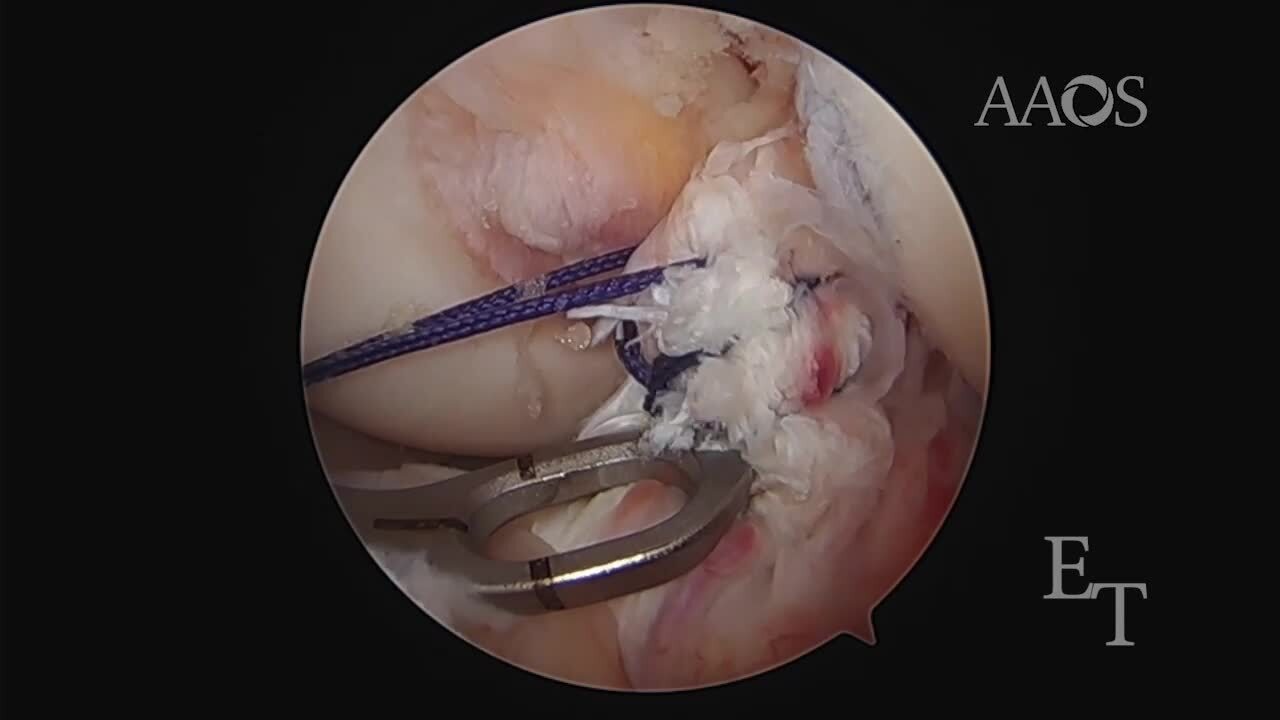
Diagnostic arthroscopy is performed to confirm a complete rupture of the ACL and the presence of a residual tibial stump. A self-retrieving suture passage device is used to whipstitch a total of six passes with No. 2 Vicryl suture from distal to proximal through the residual stump. A notchplasty followed by femoral and tibial tunnels are created in a standard fashion. An Endobutton (Smith & Nephew) soaked in a bacitracin solution is loaded with the sutures that were previously passed through the residual ACL stump, passed through the femoral tunnel, and cinched down to bone. The four suture ends that are coming from the Endobutton are then passed through the BEAR implant with the use of a Keith needle and shuttled through the tibial tunnel. The BEAR implant is hydrated with 15 mL of the patient's blood and shuttled through the anteromedial portal with the knee in full extension. The four tibial sutures passed through the graft and the tibial tunnel are passed and tensioned to the proximal tibia with the use of a second Endobutton. Standard closure is performed, and standard dressings are applied.
Results
This new surgical implant and technique have shown noninferiority to ACL autograft reconstruction with respect to International Knee Documentation Committee scores and AP laxity, with improved hamstring strength and a decreased incidence of contralateral ACL tears at 2 years postoperatively.
Discussion/Conclusion
Although initial data remains promising, future long-term studies are necessary to determine the clinical efficacy of the BEAR technique, particularly comparing it to bone-patellar tendon-bone autograft ACL reconstruction.