Management of Failed Latarjet Procedure Using a Distal Clavicular Autograft
Background
The Latarjet procedure is the preferred surgical treatment option for patients with shoulder instability who have substantial bone loss. Recurrence is rare; however, management may be challenging. Numerous revision techniques, based on soft-tissue repairs with autograft or allograft augmentation, have been developed. Autografts are associated with potential donor-site morbidity, whereas allografts may be associated with additional costs. This video discusses the use of the ipsilateral distal clavicular osteochondral autograft in a patient in whom the Latarjet procedure failed.
Indication
The indication is a failed coracoid bone block procedure with recurrent instability. Preoperative imaging studies should show an intact acromioclavicular joint with preserved coracoclavicular ligaments. This technique should not be performed if a previous lesion of the coracoclavicular ligaments was observed during coracoid harvest.
Technique Description
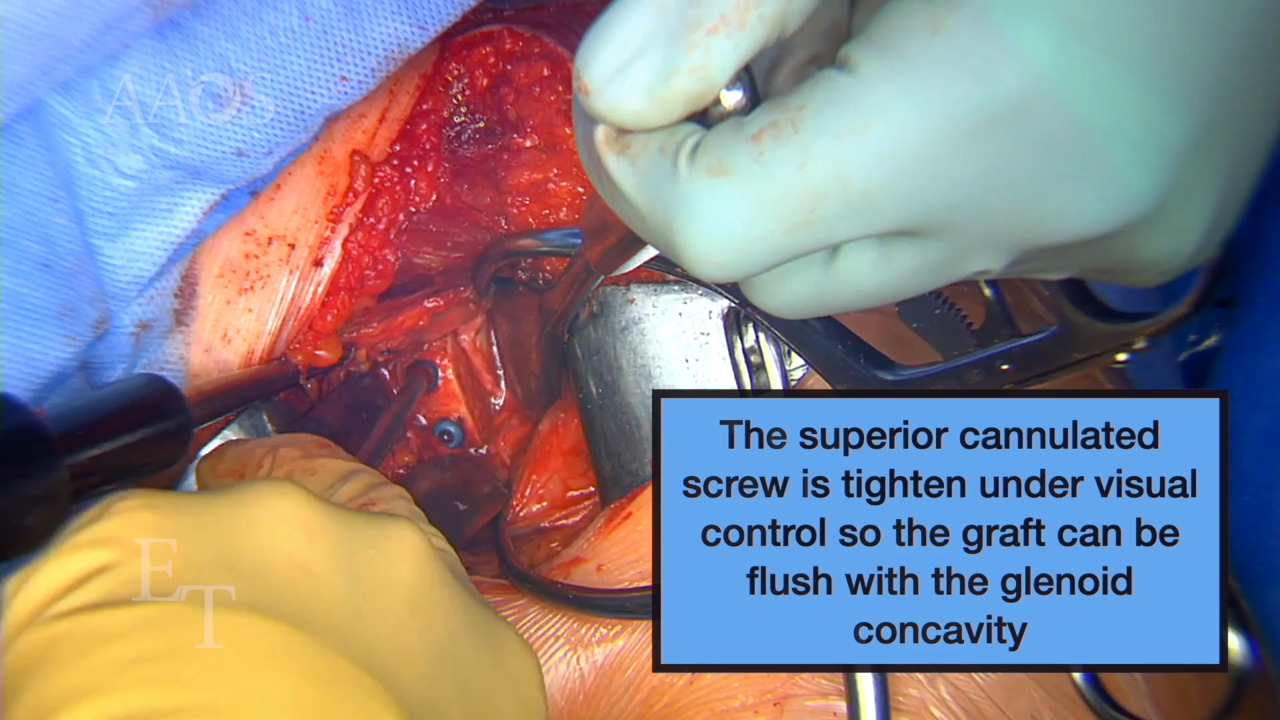
A deltopectoral approach is used and extended superiorly to access the distal clavicle end and the anterior aspect of the glenohumeral joint. A distal clavicular osteochondral autograft is harvested with the use of an oscillating saw after identifying the acromioclavicular joint with a needle to prevent resection medial to the coracoclavicular ligament insertions, which would compromise distal clavicle stability. The anterior aspect of the glenohumeral joint is exposed in a fashion similar to that during the Latarjet procedure to remove the coracoid graft remnants and any scar tissues surrounding the anterior aspect of the joint. A distal clavicular autograft is predrilled and fixed to the scapula with the use of two cortical screws. The clavicular articular surface may be used to replace the glenoid cartilage defect. In the patient in this video, the anatomy of the distal clavicle did not allow for such articular replacement.
Results
Return to daily activities was authorized after 3 weeks postoperatively. After 6 weeks postoperatively, shoulder pain decreased and no clavicle instability or donor-site complications was reported. Return to sports activity is expected in 50% of patients. CT scans showed adequate positioning of the bone block and its fusion at 3 months postoperatively.
Conclusion
In patients with recurrent shoulder instability in whom the Latarjet procedure fails, distal clavicular autograft is a reliable option to reduce donor-site morbidity and avoid additional costs. A prospective clinical study is necessary to evaluate the long-term outcomes of this technique.