Cell Therapy Combined With Bioresorbable Cement Improves Core Decompression for Management of Early Stages of Osteonecrosis of the Femoral Head
Introduction
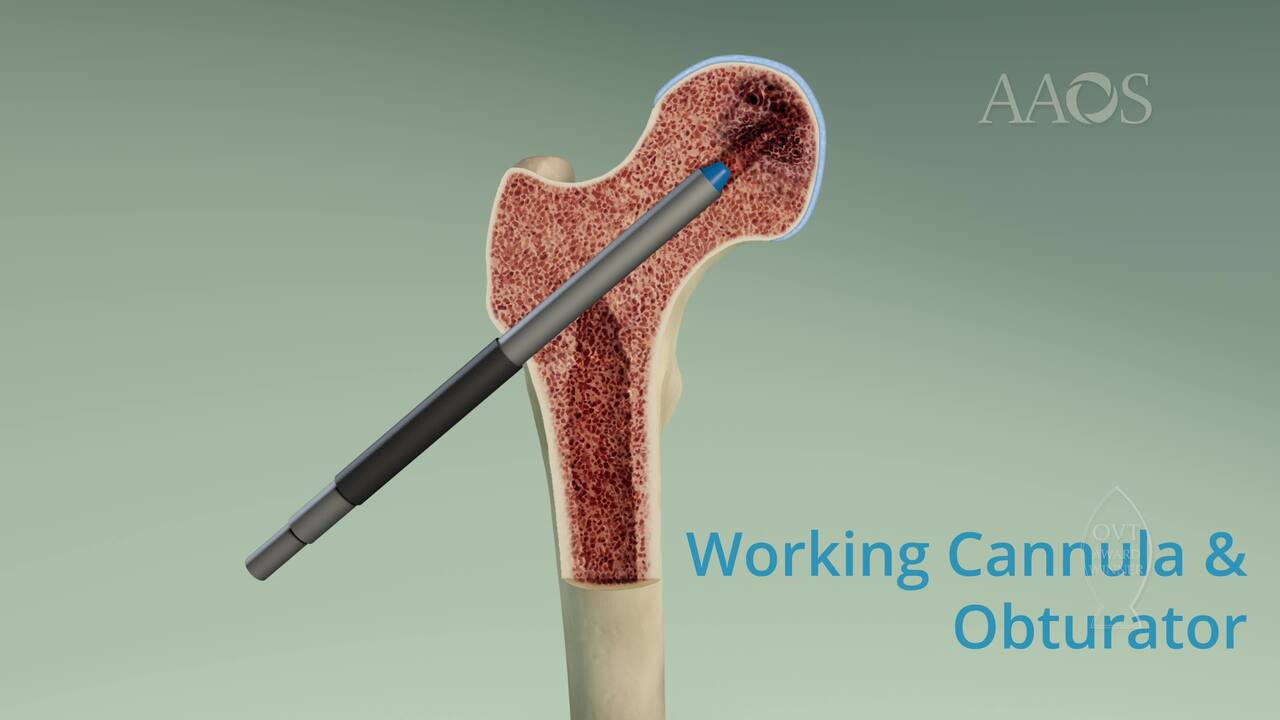
Osteonecrosis of the femoral head (ONFH) can lead to various clinical and radiographic scenarios. Management depends on the size and location of the necrotic portion. The small lesions often do not require medical or surgical management to heal, whereas bigger lesions are at risk of femoral head collapse and may benefit from surgical management and associated medical treatment. Core decompression with bone marrow aspirate concentrate (BMAC) is a surgical treatment option used in patients with early stages of ONFH. It prevents femoral head collapse and slows disease progression, delivering osteoprogenitor cells with the aim of trabecular bone and microvasculature reconstitution.
Material and Methods
A retrospective analysis was conducted on 21 patients (30 femoral heads) with ONFH who were treated between January 2016 and January 2022. Patient demographics, comorbidities, body mass index, smoking status, etiology, lesion grade based on Association Research Circulation Osseous, preoperative and postoperative Harris Hip Scores (HHS), and radiographic progression were collected. Patients underwent clinical and radiographic follow up at 1, 6, and 12 months postoperatively. Mean follow-up was 20 months (range, 12 to 36 months).
Results
A total of 21 patients (14 males, 7 females) with a mean age of 36 years (range, 24 to 50 years) were treated via core decompression with BMAC and cement bone substitute. Of the 30 femoral heads, 12 were classified as stage I, and 18 were classified as stage II. Etiology was long-lasting steroid therapy in 10 patients, alcohol abuse in four patients, sickle cell anemia in two patients, and idiopathic etiology in five patients. The mean Harris Hip Score increased from 53 (range, 41 to 61) preoperatively to 80 (range, 72 to 86) at 6 months postoperatively and to 88 (range, 82 to 94) at 12 months postoperatively. At 1-year follow-up, radiographic progression was observed in only four patients: two patients shifted from stage I to stage II, and two patients shifted from stage II to stage IIIb. No complications occurred intraoperatively or postoperatively. Conversion to total hip arthroplasty was performed in one patient during follow-up.
Discussion
Core decompression with cell therapy resulted in a relatively superior result in radiographic progression compared with nonsurgical management. BMAC was found to decrease disease progression and conversion to total hip arthroplasty and was associated with better functional outcome scores compared with core decompression alone; however, the combination of core decompression and BMAC is not effective in patients with large lesions, and additional studies are necessary to verify the effectiveness of BMAC. With regard to quantity, the use of 20 mL of BMAC and 10? magnitude bone marrow mononuclear cells likely is associated with better results.
Conclusion
Core decompression is an effective and safe method for the management of ONFH. The combination of core decompression with BMAC in patients with pre-collapse stages of the disease is beneficial with regard to improving function scores, reducing the radiographic progression of disease, and decreasing the need for total hip arthroplasty. Based on current evidence, BMAC may be an effective treatment option for delaying disease progression or reducing disease development; however, additional studies with high-level evidence are necessary.