Surgical Hip Dislocation for Synovial Chondromatosis
Background
Synovial chondromatosis is a rare, progressive disease that results in loose bodies that can cause considerable pain, decreased range of motion, and intra-articular wear. Surgical treatment in the form of a surgical hip dislocation or hip arthroscopy typically is indicated in patients with extensive intra-articular involvement of the hip for symptom relief and joint preservation. The indications for surgical dislocation have changed over time; however, surgical dislocation remains an effective treatment option for patients with considerable intra-articular pathology.
Purpose
This video provides an overview of surgical hip dislocation in a patient with extensive intra-articular loose bodies secondary to synovial chondromatosis.MethodsThe history and indications for surgical dislocation are presented. The patient is a 16-year-old girl with no important medical history. She presented with severe left hip pain and difficulty with ambulation, which had persisted for 1 year. On physical examination, the patient walked with an antalgic gait and was tender to palpation over the psoas muscle. Hip range of motion was limited to 0° to 90° and was associated with considerable pain. She also had a positive flexion, abduction, external rotation test. Radiographs and CT scans of the left hip revealed a cam lesion with extensive posterior extension and numerous intra-articular loose bodies, with limited arthritic changes. After a thorough discussion of the risks, advantages, and prognosis, the patient elected to undergo surgical hip dislocation with removal of the loose bodies and contouring of the femoral head/neck junction.
Results
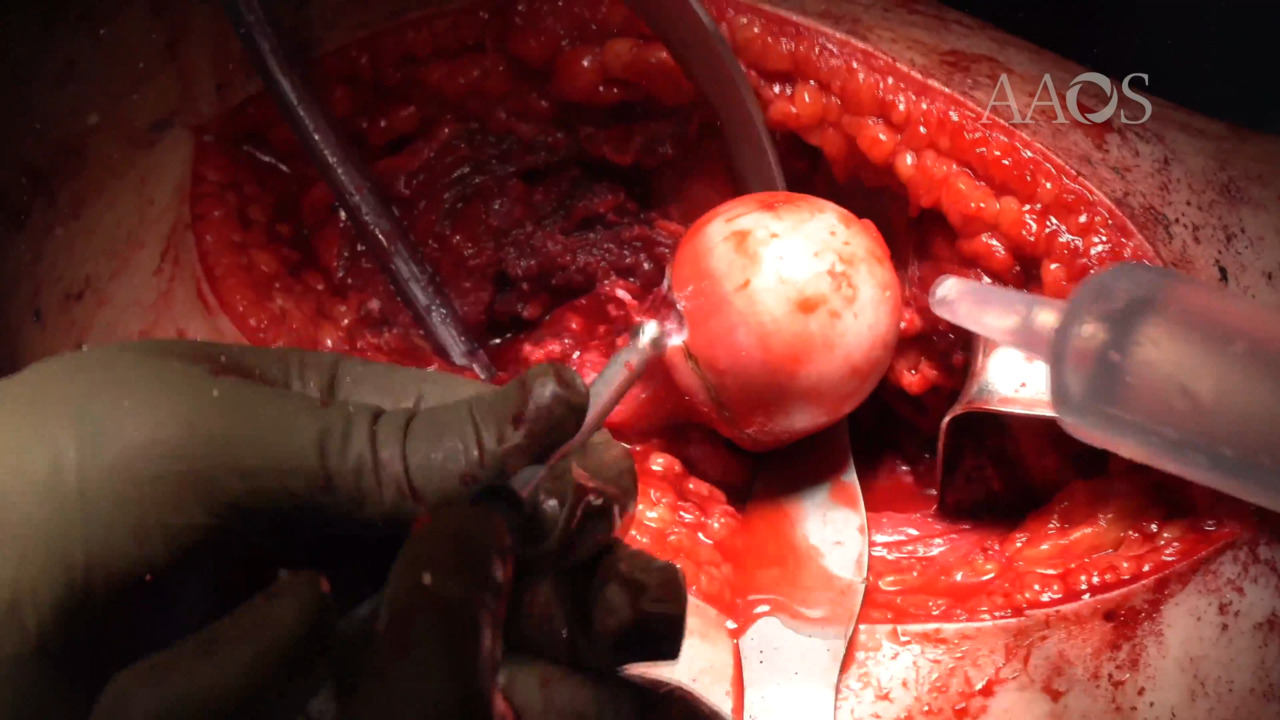
The patient was placed in the lateral decubitus position, and a straight lateral incision was centered over the greater trochanter. Proximally, the interval between the gluteus maximus and the tensor fascia lata was developed, exposing the underlying gluteus medius muscle. Distally, the iliotibial band was incised. The retro-trochanteric space was exposed, and the interval between the piriformis tendon and the gluteus minimus was developed. Careful attention was taken to avoid the medial circumflex artery. A step-cut osteotomy of the greater trochanter was then performed. The osteotomy fragment was retracted anteriorly with the vastus lateralis and the hip abductors. With progressive abduction, flexion, and external rotation, the anterior hip capsule was visualized, and a Z-type capsulotomy was performed, exposing many small intra-articular ossicles. The femoral head was then dislocated. All the loose bodies were removed, and the joint was thoroughly irrigated. A femoral osteoplasty was then performed to remove the cam deformity. A small hole was subsequently drilled into the femoral head, confirming bleeding vascularized bone. The hip was reduced and determined to be stable through full range of motion, with no signs of residual impingement. Intraoperative fluoroscopy was used to confirm removal of all the loose bodies and adequate resection of the cam deformity. The capsulotomy was subsequently closed, and two 4.5-mm fully threaded cortical screws were used to secure the step-cut osteotomy fragment. The patient was allowed to partially bear weight with the use of crutches and was instructed to maintain trochanteric hip precautions. At 4 weeks postoperatively, the patient reported improved pain; had a negative flexion, abduction, external rotation test; and was allowed to bear weight as tolerated with the use of one crutch. The incision appeared well healed, and radiographs demonstrated stable fixation of the osteotomy site without interval displacement.
Conclusion
Surgical hip dislocation is a valuable tool for the management of intra-articular pathology. Patients with primary synovial chondromatosis have experienced successful resolution of symptoms after surgical hip dislocation, with low rates of recurrence at latest follow-up; however, substantial risks are associated with the procedure, which may be technically demanding. In-depth knowledge of the anatomy of the medial circumflex artery is essential, and care must be taken to avoid occult intra-articular damage.