In-situ Fixation and Imhäuser Intertrochanteric Osteotomy for Chronic Severe Slipped Capital Femoral Epiphysis
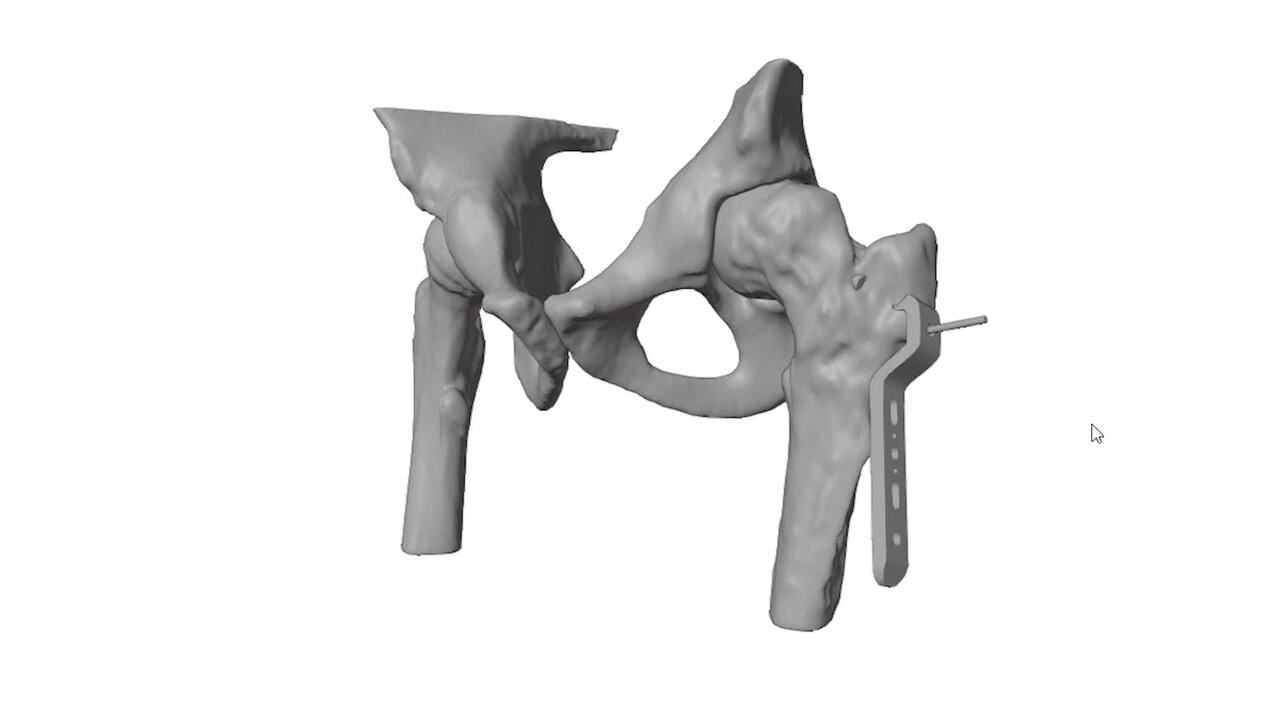
Background: Slipped capital femoral epiphysis (SCFE) is a condition where the femoral head slips posteriorly and inferiorly relative to the femoral neck through the growth plate. SCFE is relatively rare, affecting 2 to 3 individuals per 100,000, with a mean age of onset between 10 and 14 years. Bilateral involvement occurs in 18% to 50% of cases. Most cases occur without any preceding injury, some patients do recall a minor or nonspecific traumatic event occurring weeks or months before presentation. A few patients even note an acute and more severe mechanism of injury. In rare instances, SCFE can occur in patients recovering from a high-energy femoral neck fracture that was treated with internal fixation. Based on the duration of symptoms, SCFE can be classified into three categories: acute, chronic, acute-on-chronic. SCFE can present as stable or unstable. Managing moderate to severe SCFE is complex. The key challenge is choosing between intra-articular and extra-articular osteotomy. Intra-articular osteotomy offers the best correction but is technically demanding and has a higher risk of avascular necrosis (AVN) and major complications. Extra-articular intertrochanteric osteotomy (ITO) is easier and has a lower risk of complications but may result in incomplete correction and residual deformity. This can lead to femoroacetabular impingement, early osteoarthritis, and potentially necessitate total hip replacement (THR).Aim: The aim of this video is to illustrate the steps of the Imhäuser ITO combined with “in-situ” fixation (ISF) and osteochondroplasty of the femoral head. Additionally, we demonstrate the use of Virtual Surgical Planning and 3D-Printed cutting guides to fasten and enhance the precision of the surgical procedure.Methods: We present the case of a 15-year-old male with a femoral neck fracture treated with closed reduction and internal fixation. A one-month follow-up radiograph showed satisfactory fracture healing but mild SCFE onset, which worsened three months later. Based on current literature, we planned an Imhäuser ITO combined with ISF and osteochondroplasty of the femoral head, using virtual surgical planning and 3D-printed cutting guides. The video illustrates the step-by-step Imhäuser ITO, preoperative 3D planning, and design of patient-specific templates and cutting guides. It also covers clinical-radiographic diagnostics, surgical principles, our experience with moderate and severe SCFE, and key literature evidence.Results: Between 2015 and 2023, 14 patients with moderate to severe SCFE (10 males, 4 females; mean age: 13.3±1.1 years) underwent a combined procedure involving ISF and Imhäuser ITO. The mean preoperative Southwick angle was 75° ± 16° (range 45°-101°), which improved by an average of 55° (95% CI: 47°-63°; p < 0.0005) postoperatively. The mean follow-up was 6 ± 1.9 years (range: 1-9). No major complications or re-operations were observed. At the most recent follow-up, the mean Hip Disability and Osteoarthritis Outcome Score (HOOS) was 97 ± 6 points (range 83-100).Conclusions: The Imhäuser ITO, combined with ISF and osteochondroplasty, is an effective surgical option for chronic severe SCFE. The risk of AVN, major complications, or early conversion to THR is very low. The use of 3D preoperative planning and 3D-printed surgical guides in the Imhäuser ITO can significantly enhance the accuracy of correction and reduce surgical duration compared to the classic approach. Additionally, the residual intra-articular bump can be safely and effectively removed concurrently through an anterolateral approach.