Soft Tissue Surgical Technique: Obligate Dislocation of the Patella in Children
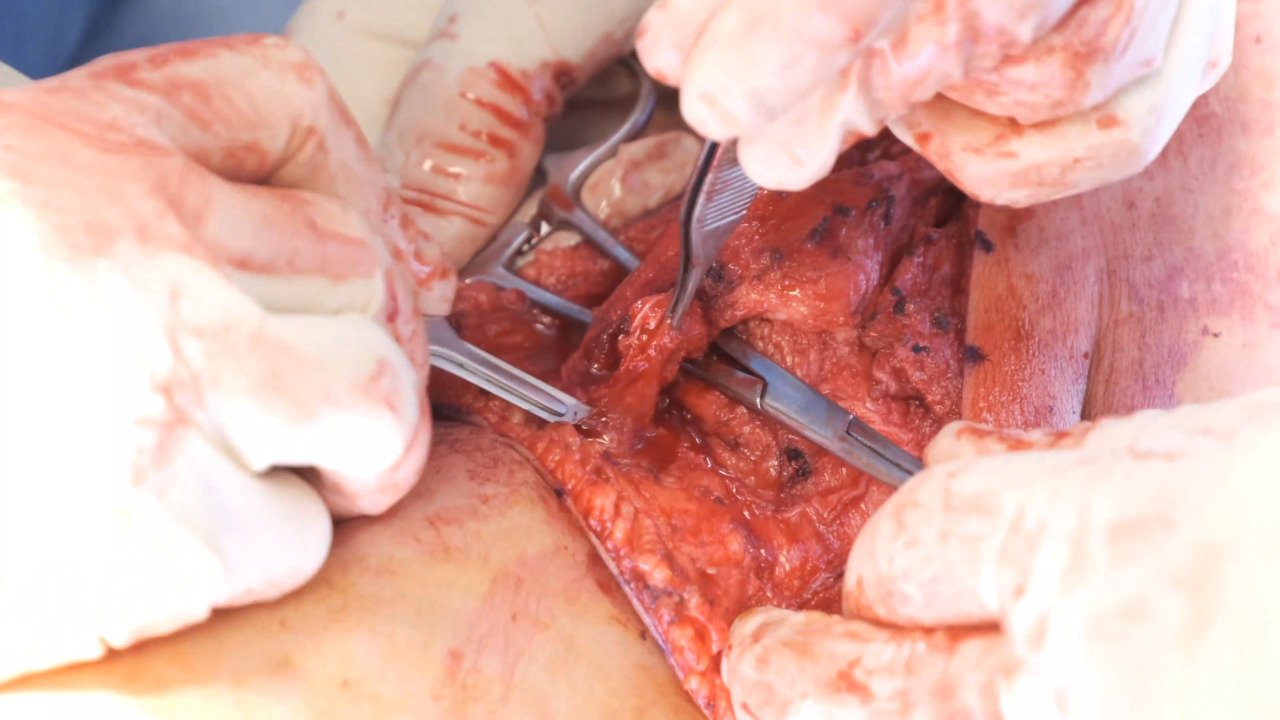
Summary: Obligate dislocation of the patella (ODP) is part of a spectrum of patella dislocation ranging from intermittent to irreducible. Associated orthopedic deformities can include femoral retroversion, genu valgum, calcaneovalgus foot deformity, or tibial torsion. Patella dislocation, especially more severe presentations, can be associated with other genetic conditions or syndromes. Severe patella dislocation deformities are diagnosed clinically at birth or in childhood. Severity of the condition is variable; the patient may not experience significant disability or may not be able to ambulate. As the patient gets older, the patella can become harder to reduce or remain permanently dislocated. The contraction of the soft tissue around the knee, in some cases, causes a flexion contracture, preventing standing or ambulation. Definitive treatment for ODP is surgery, and the decision for type of surgical procedure is determined by skeletal maturity. Skeletally immature patients undergo soft tissue only procedures. Current literature regarding patella dislocation is limited, and video demonstration of a soft tissue procedure for skeletally immature soft tissue correction is lacking. The technique described here is not present in the video literature. Surgical correction of two 7-year-old skeletally immature patients with ODP is shown using lateral release, patella tendon split transfer (medial side only), VMO advancement, and Z lengthening of the quadriceps tendon. Both patients did well post operatively with initiation of early weight bearing and early range of motion. At 6 months, one was back to full activity for the first time in his life. Many pearls can be gleaned from this surgery. Most notable pearls include taping a sandbag to the table to help position the knee to 60 degrees of flexion to aid in proper tensioning while reattaching tendons, be generous with lateral release if tightness is encountered but careful not to damage the lateral meniscus, address quad shortness by lengthening, utilize up to 100% VMO advancement, and move the medial half of the patella tendon more medially to prevent torque on the patella while maintaining the lateral half intact. The authors believe this is an excellent contribution to the literature for those encountering patients with this spectrum of patella dislocation disorders.