Minimally Invasive Bridging Plate Osteosynthesis for Extra-articular Distal Humeral Shaft Fractures: From Anatomy To Surgical Treatment
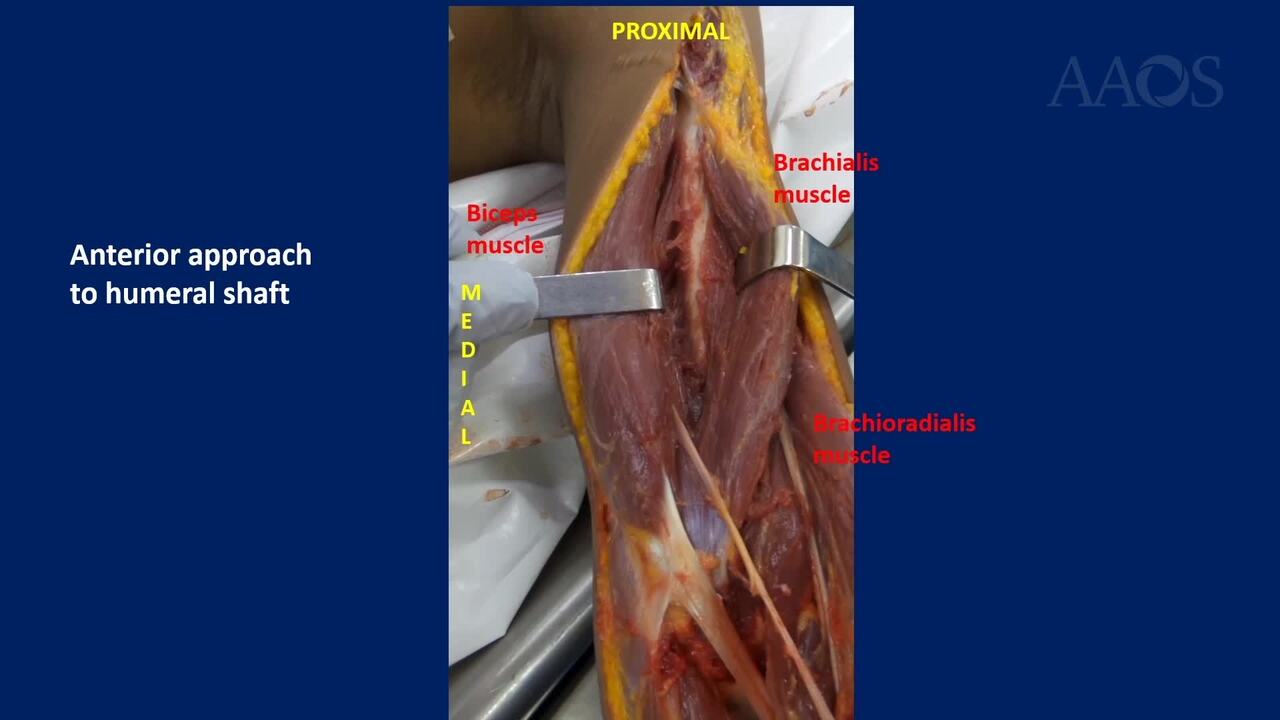
Introduction: Humeral diaphyseal fractures correspond to approximately 3% of fractures in trauma. Clinically, it presents bimodally according to age; A first group occurs in male patients in the 3rd decade, usually due to traffic accidents, and a second group in female patients in the 7th decade of life due to low bone mineral mass in low-energy traumas. It is clearly accepted in the literature that non-surgical treatment of humerus shaft fractures continues to be the standard of management, since nonunion rates are very low and the functional results in the shoulder and elbow are good. Fractures of the distal third of the humeral shaft represent a different scenario than midshaft or proximal shaft fractures due to the rates of malunion in the coronal plane when non-surgical management is performed, specifically varus angulations of more than 10 degrees in a significant number of patients in addition to higher rates of elbow stiffness due to immobilization time. Surgical treatment alternatives for fractures of the distal third of the humerus have been classically described with posterior approaches to expose the focus of the fracture and performing neurolysis of the radial nerve, but this has increased deperiostization and nonunion rates. Anterolateral approaches with visualization and exposure of the radial nerve are used as a treatment for the fixation of the most distal fragments, including fixations with two plates in patients with low bone mineral mass for greater fixation. These are surgical alternatives described that increase the difficulty of the procedure as well as that the risks of praxis or nerve injuries. Minimally invasive methods have been developed for the osteosynthesis of humeral diaphyseal fractures, reporting good clinical results with reproducible outcomes.Purpose: To show the macroscopic anatomy of the shoulder and anterior arm up to the elbow, in cadaver lab, with emphasis on the muscular and nervous anatomy and its relationship with the humeral diaphysis, and a video of the osteosynthesis with a locking compression plate of a distal humerus fracture in a cadaver through a proximal and a distal incision, a measurement of the distance of the plate to the radial nerve, the lateral humeral cortex and the proximal edge of capitellum is performed. Additionally, we investigated the outcomes of surgical treatment of this type of injury in our patients.Methods: A video showing the gross anatomy of the anterior shoulder and arm and the surgical treatment of simulated distal-third diaphyseal fractures of the humerus fracture with locking compression plate through a proximal and a distal incision in cadaver lab is presented. In 8 cadaveric arms, a transverse fracture of the distal third of the humeral shaft was recreated by a direct posterior approach using a saw; the plate was pre-bent to achieve adequate adaptation to the anterior cortex of the distal humerus. Through the distal incision, a blunt dissection is performed in the center of the brachialis muscle in the same orientation of its fibers until the distal humeral shaft is exposed; the second incision is made in the proximal third of the arm, approaching the humeral shaft through the deltopectoral interval. The plate is introduced in a retrograde manner from distal to proximal and and the plate is fixed with 3 or 4 screws at the distal end and 2 or 3 screws at the proximal end. A measurement of the distance of the plate to the radial nerve, the lateral humeral cortex and the proximal edge of capitellum is performed in all cadavers. 10 patients with displaced fracture of the distal third of the humeral shaft who underwent to this surgical procedure were evaluated. The arm was immobilized in a sling for 2-3 weeks postoperatively and passive exercises were started on the first postoperative day and active-assisted range of motion at 1 postoperative week. The outcomes were assessed at a mean follow-up of 33 months (range, 9 to 61 months) through the Mayo Elbow Performance Score (MEPS), American Shoulder and Elbow Surgeons Score (ASES), Visual Analogue Scale (VAS) of pain and patient satisfaction.Results: 10 patients (6 men, 4 woman) with a mean age of 31.8 years (range, 19 to 61 years; standar deviation [SD] &[plusmn] 12.2 years) were included in the study. All the patients had displaced fracture of the distal third of the humeral shaft. At the end of the follow-up, the mean of Mayo Elbow Performance Score (MEPS) was 89.5 (range, 79 to 100; standard deviation[SD] &[plusmn] 10.12), the American Shoulder and Elbow Surgeons Score (ASES) was 92 (range, 82 to 100; standard deviation [SD] &[plusmn] 8.08) and the Visual Analogue Scale (VAS) of pain was 1 (range, 0 to 3; standard deviation [SD] &[plusmn] 1.13) . The patient satisfaction was 10 in all patients and fracture union was found in all patients. In cadaver lab, the minimum distance from the distal part of the plate to the proximal edge of the capitelllum was 10 mm, which does not produce a mechanical limitation to elbow flexion; the minimum distance from the lateral part of the plate to the radial nerve was 10 mmConclusion: Distal humeral shaft fractures have an increased risk of residual varus deformity and decreased range of motion at the elbow with non-surgical functional management. Minimally invasive plate osteosynthesis for extra-articular distal humeral shaft fractures treatment using a bridging plate is a very good alternative for the treatment. Clear knowledge of anatomy is essential to reduce the risk of iatrogenic nerve injuries.