Total Hip Arthroplasty with Subtrochanteric Osteotomy for Congenital Hip Dysplasia
Background: Adult hip dysplasia occurs in approximately 3 to 5% of adults in the United States. Risk factors include female sex, breech presentation, first born child, and a family history of hip dysplasia. The Crowe classification is a four-part system that is used to classify dysplasia based on femoral head displacement. Pelvic osteotomies or hip resurfacing are treatment options for less severe cases of dysplasia. In more severe cases of dysplasia, total hip arthroplasty remains the main stay option for pain relief and improved ambulation.
Purpose: This video provides an overview and reviews a case presentation of a patient with hip dysplasia who underwent a total hip arthroplasty with a subtrochanteric osteotomy.
Methods: The patient history and indications for total hip arthroplasty with a subtrochanteric osteotomy are presented. The patient is a 45-year-old male with Crowe IV left hip dysplasia. He has had difficulty and pain with ambulation. He has a 5 centimeter leg length discrepancy. Radiographs of the pelvis and hip demonstrate Crowe IV hip dysplasia with complete native acetabulum deficiency and a superior pseudo-acetabulum.
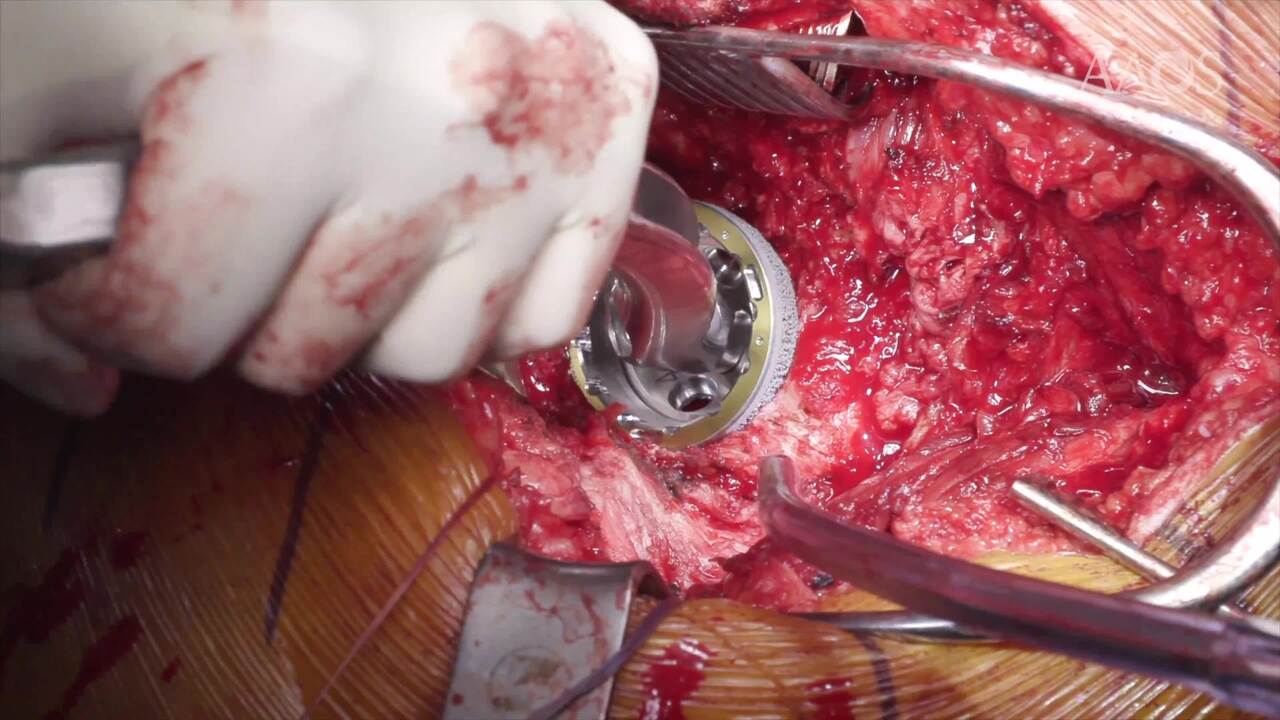
Results: A standard posterolateral incision was made and soft tissue dissection was carried down through the IT band. Soft tissue distal to the lesser trochanter where released off of the femur in preparation of the osteotomy. The femoral neck was cleared of soft tissue and a femoral neck cut was made. The femoral osteotomy was marked about 2cm distal to the lesser trochanter. After reaming the femur, a trial was then placed in the femoral canal. Fluoroscopy was used to aide in identifying the native acetabulum. We then sequentially reamed into anatomic position being careful not to over ream the superior dome and anterior wall. A multihole cup was impacted into position and multiple screw holes were drilled and screws were placed.
We then returned to the femur and measured the distal portion of the osteotomy. A trial head and neck were placed, and the proximal femur was reduced into the cup. Once the length of the osteotomy was confirmed and the rotation of the femur was marked, the distal osteotomy was made. The hip was then reduced and stability was assessed. The sleeve of the stem was impacted followed by the stem into the distal femoral shaft. The femoral osteotomy fragment autograft was wrapped around the osteotomy site and cabled. The final head was impacted into place and the hip was reduced. Stability was then assessed and the hip was found to be stable and free of impingement. At 3 months postoperative visit, the patient was ambulating 8-10 city blocks. His incision was well healed, and radiographs demonstrated stable implants without evidence of loosening or subsidence.
Conclusion: Total hip arthroplasty with a subtrochanteric osteotomy can provide improved pain and function in patients with severe hip dysplasia. Patients report improvement in Harris Hip Score, a reduction in the need for assistive devices, and improved leg length discrepancy. Appropriate preoperative planning and intraoperative radiographs are needed to ensure appropriate placement of the acetabular shell and an adequate femoral osteotomy.