Trigger Wrist and Anatomy of the Extended Carpal Tunnel Approach
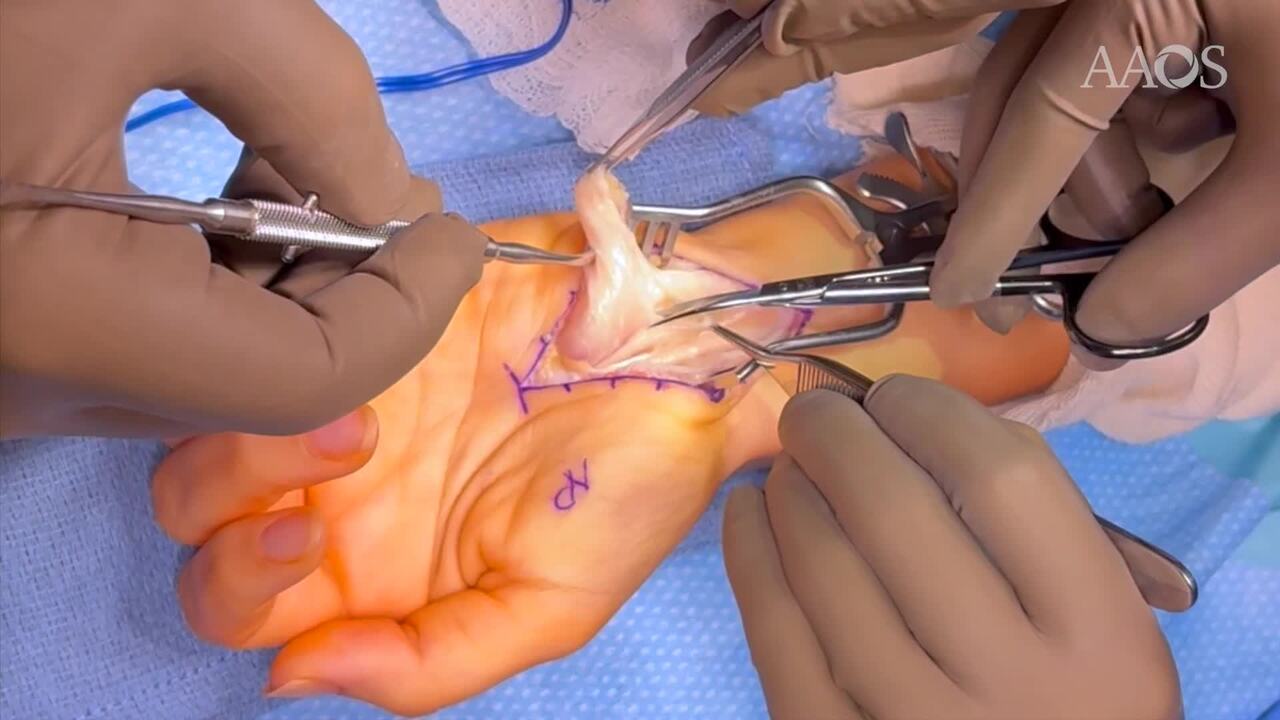
Trigger wrist is a rare condition characterized by painful clicking, locking, or snapping sensations during finger or wrist motion. Unlike trigger finger, trigger wrist results from pathology affecting structures within or around the carpal tunnel. Few case reports on this phenomenon exist, with previous reports describing the compressive etiologies as tumors (fibromas, lipomas, rheumatoid nodules), anomalous muscle bellies (hypertrophied FDS), or fibrotic changes.A 31-year-old female presented with progressive left-hand numbness and tingling in the median nerve distribution; and a locking and popping sensation at the wrist when attempting to make a fist. Physical examination revealed triggering at the distal forearm just proximal to the carpal tunnel between the flexor tendons and ulnar neurovascular bundle. Radiographs revealed no significant findings. Wrist ultrasound demonstrated a heterogeneous hypoechoic mass insinuated between the third and fourth flexor tendons. MRI demonstrated a well-defined enhancing mass within the carpal tunnel, suggestive of a TGCT. EMG demonstrated median nerve neuropathy with evidence of sensory and motor axon loss. Surgical intervention was pursued due to persistent symptoms and mechanical dysfunction. A volar approach to the wrist using a Bruner style incision was made proximally across the wrist, extending to the distal forearm. The transverse carpal ligament was released and there was significant compression about the median nerve secondary to the mass. Exploration revealed a heterogeneous orange/pink mass with surrounding extensive tenosynovitis. Intraoperatively, a firm, encapsulated mass measuring approximately 5 x 3 cm was found compressing the median nerve and flexor tendons. There was a hourglass type deformity of the median nerve and epineural release was performed. The mass was completely excised without complications. Histopathology confirmed the diagnosis a tenosynovial soft tissue mass with hyperplastic changes. Postoperatively, the patient experienced complete resolution of the locking and popping sensations, as well as improvement in sensory symptoms. At 1-week follow-up, no recurrence was observed, and the patient began OT. This case highlights the importance of considering trigger wrist in patients presenting with mechanical symptoms alongside CTS. According to the classification system of Suematsu et. al, this case belongs to type A (caused by a tumor). MRI plays a crucial role in identifying space-occupying lesions within the carpal tunnel and further literature review of mass size may assist in better understanding biomechanics of the wrist triggering phenomenon. Early recognition and surgical excision can lead to favorable outcomes, preventing misdiagnosis and unnecessary treatments.