Combined Open Latissimus Dorsi/teres Major and Lower Trapezius Tendon Transfer with Achilles Allograft for a Massive Irreparable Rotator Cuff Tear
Introduction: A 54-year-old right-hand-dominant male presented with chronic right shoulder pain that was found to be consistent with tears of the supraspinatus, infraspinatus, and subscapularis. Magnetic resonance imaging demonstrated a massive tear of the subscapularis, diseased biceps tendon, acromioclavicular joint arthrosis, and mild glenohumeral degeneration. In addition to age-related degenerative changes, repeated overhead activity can cause full-thickness tears of the rotator cuff. Range of motion of the affected shoulder can be impacted, leading to limited external rotation and elevation of the shoulder. Due to the size of the tear, these deficits can be addressed effectively through an open surgical approach.Indications:The decision was made to proceed with an open repair of the rotator cuff. To restore full rotator cuff force, a lower trapezius tendon transfer and concomitant latissimus dorsi and teres major tendon transfer were indicated. Combining the transfer of the latissimus dorsi and teres major restores external rotation, while transferring the lower trapezius tendon improves the strength of abduction and external rotation. The latter depends on an Achilles tendon allograft, which serves as a bridge between the greater tuberosity and lower trapezius. Ultimately, this procedure would optimize function while reducing pain over time.
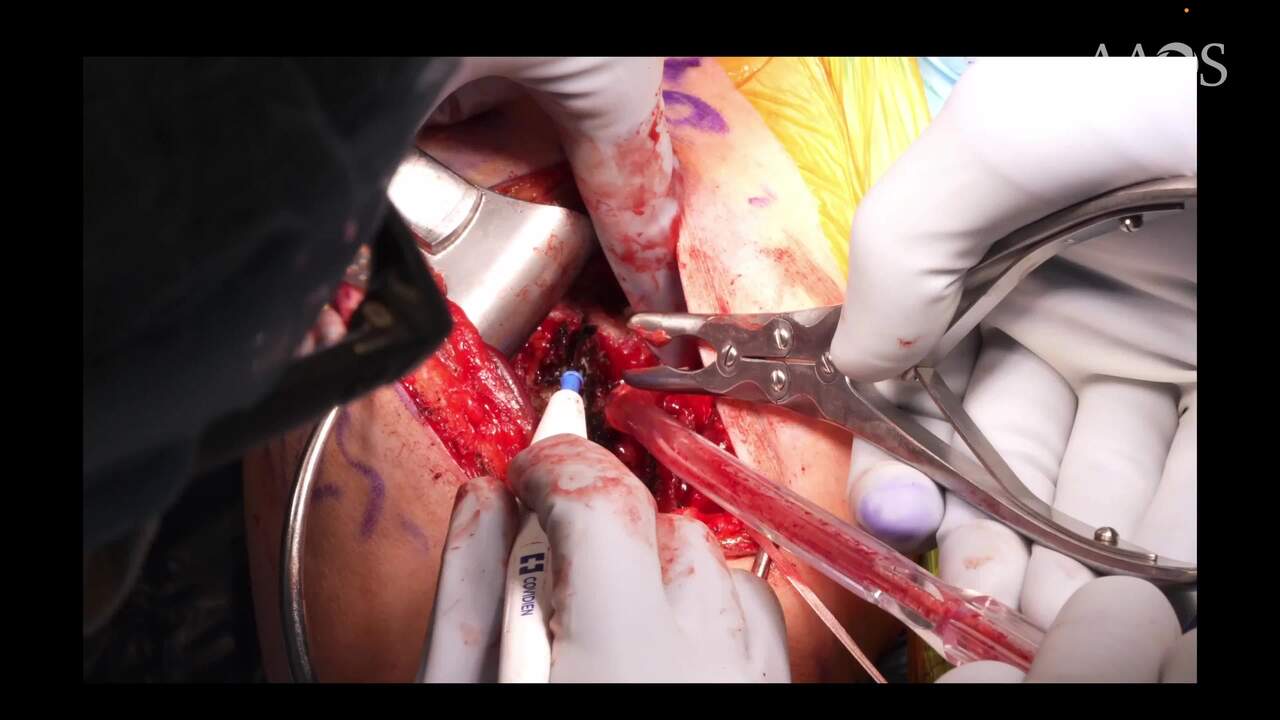
Technique: Consent for the aforementioned procedure was obtained. The correct shoulder was marked as the operative site, and a timeout was performed by the team. The patient was placed in the beach chair position. The right upper extremity was then prepped and draped following sterile protocol. A standard deltopectoral incision was performed, using the inferior portion and upper aspect of the arm. Entrance into the deltopectoral fascia revealed significant scarring and adhesions, which were subsequently dissected. Additionally, substantial scarring and adhesions to the humerus were dissected. Two #2 sutures were used for the muscle transfer portion of the case. Following the trapezius tendon transfer, attention was turned to fixation of the subscapularis and lat/teres transfer. A thick alloderm was used to extend the transfer. Several #5 sutures were used to achieve good fixation.The lower trapezial tendon transfer with Achilles tendon allograft, as well as the biceps tendon transfer to the superior greater tuberosity, was started by incising horizontally along the medial aspect of the scapular groove. The trapezial muscle coursed superiorly and inserted onto the medial border of the scapula, so the inferior border of the muscle was dissected. To protect the spinal accessory nerve, a plane was created between the middle and inferior portions of the trapezius muscle. The Achilles allograft was then prepared, placed over the inferior trapezial tendon, and sutured in. Finally, the site was thoroughly irrigated and closed in a layered fashion.
Discussion/Conclusion: In this case, open rotator cuff repair with combined latissimus dorsi, teres major, and lower trapezius tendon transfer resulted in satisfactory short- and long-term clinical outcomes. This included well-controlled pain, as well positive changes in patient-reported outcomes measures and range of motion on physical exam. The patient continues to progress appropriately. This joint-preservation technique, also known as the “parachute” technique, is a reliable surgical option for younger, active patients with irreparable subscapularis and posterosuperior rotator cuff tears.