Vertebral Column Resection in the Management of Congenital Thoracic Kyphosis: Treatment Principles and Surgical Technique
Thoracic hyperkyphosis is a sagittal spinal deformity characterized by an increased magnitude of thoracic kyphosis or abnormal location of its apex. This can result from various etiologic factors, including congenital segmentation or formation defects, developmental conditions such as Scheuermann’s disease, inflammatory, metabolic, or post-traumatic causes like osteoporotic fractures, and iatrogenic origins following surgery, irradiation, or junctional failure after deformity correction. In severe cases, the gold standard for surgical correction for thoracic hyperkyphosis is posterior spinal fusion associated with different types of vertebral osteotomies.
Three key factors should be evaluated: the magnitude, the shape, and the flexibility of the deformity. Magnitude is measured using the Cobb angle. The shape reflects the number of vertebral bodies involved in the curve, distinguishing between sharp, short-radius curves and rounded, large-radius ones. These two elements can be combined into the Deformity Angular Ratio (DAR), calculated as the Cobb angle divided by the number of vertebrae included. Flexibility describes how much the curve can be corrected through postural changes, typically assessed with supine X-rays with a bolster at the apex of the deformity. Three-column osteotomies such as pedicle subtraction osteotomy (PSO) are indicated for sharp curves with high DAR, or for rigid, rounded deformities with low DAR. PSO can provide up to 30 degrees of angular correction in the lower thoracic spine, but its corrective potential decreases cranially due to the smaller pedicle height. When the required correction exceeds the capacity of a single PSO in sharp deformities, a Vertebral Column Resection (VCR) is indicated. The aim of the present work is to present the results of VCR for the treatment of severe sharp congenital thoracic hyperkyphosis focusing on the technique and its safety and efficacy. This was a retrospective study. We included all the patients who underwent VCR for severe sharp thoracic hyperkyphosis between January 2019 and June 2024. All patients received one-stage posterior spinal fusion and posterior-only VCR. All patients received pre-operative radiographical evaluation with full spine standing x-rays in postero-anterior and lateral view and lateral view and CT scan of the thoraco-lumbar spine. The fusion area was selected to obtain at least four anchor points proximally and distally to the planned osteotomy site. The selection of lowest instrumented vertebrae was done following the criteria described by Cho et al. Sensory and Motor evoked potentials were monitored. All the patients received a post-operative full spine standing x-ray in postero-anterior and lateral view in order to evaluate post-operative radiographical outcomes. All of the radiographic measurements, aimed to assess the deformity correction, sagittal and coronal alignment, were obtained by the same experienced surgeons who performed the surgeries. SRS-22 questionnaire was submitted pre-operatively and at the last follow-up, in order to detect the satisfaction of the patients with the surgical treatment. A total of 9 patients (7 females, 2 males) were included, with a mean age of 16.8 years (range 12-25 years, sd: 5.6 years) and a mean follow-up of 26.2 months (range 12-38 months). The included patient could be classified: 2 as failure of formation (sagittal wedge vertebra and sagittal hemivertebra), 3 as failure of segmentation (anterior intervertebral bony bar), 4 as mixed abnormalities of segmentation and formation. Estimated blood loss, surgical time and length of stay were 1534.2 ± 730.4 mL, 320.8 ± 85.3 minutes and 10.5 ± 4.2 days, respectively. Deformity angle, T1-T12 Thoracic Kyphosis, L1-S1 Lumbar Lordosis and Sacral Slope improved from 79° to 30°, from 61° to 40°, from 95° to 54°and from 41° to 33°, respectively. Five post-operative complications were reported, 2 superficial wound dehiscence treated with surgical debridement, antibiotics and implant retention, 2 pneumothoraxes, 1 dural tear. Severe, sharp thoracic hyperkyphosis may lead to sagittal spinal malalignment, impaired aesthetic appearance, pain, early degenerative changes in the lumbar and cervical spine, as well as neurological complications. Vertebral osteotomies have been classified by Schwab et al., and in cases of sharp, stiff deformities, they may represent the only surgical strategy capable of achieving proper correction.
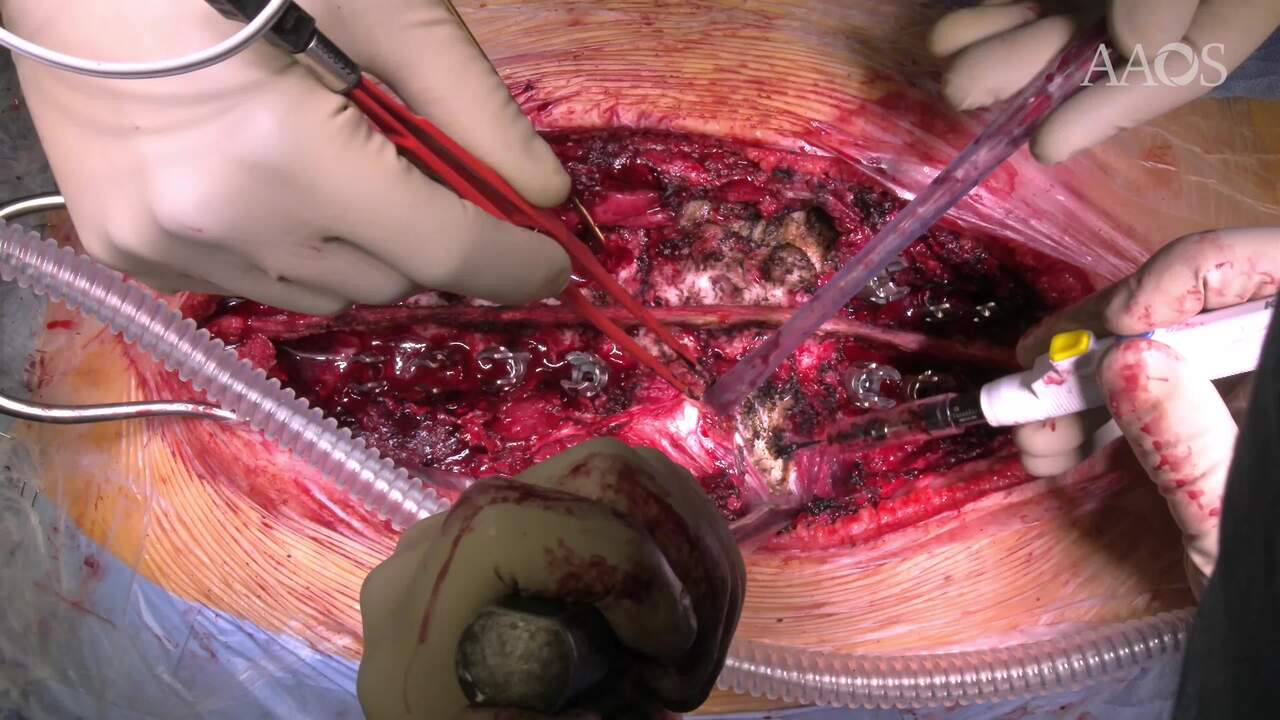
Grade 5 osteotomies, also known as VCR, offer a high corrective potential and allow for the correction of focal and/or multiplanar deformities; however, they are associated with risks such as significant bleeding, neurological injury, and dural tears. The closure of the osteotomy is the most difficult part of the surgery, as this is when most neurological complications may occur. A domino rail system construct allows the corrective forces to be distributed over a greater number of anchor points, providing increased stability to the destabilized spine during closure. This results in a reduced risk of screw pull-out and greater control over the corrective phase, achieved through sequential compression maneuvers and in situ rod contouring to reduce local kyphosis. Although technically demanding, VCR via posterior-only has proven to be an effective and safe option for correcting severe sharp thoracic hyperkyphosis —such as congenital kyphosis—when performed by experienced surgeons.