Lateral Extra-articular Tenodesis via the Modified Ellison Technique
Background: ACL injuries are common amongst athletes, and literature suggests that augmenting a primary ACL repair with a lateral extra-articular tenodesis (LET) can lead to significant reduction in graft failure and rupture rate. Traditionally, the LET is done via the modified lemaire technique, in which a strip of IT band is shuttled deep to the LCL and attached to the lateral femoral condyle. An alternative technique, known as the modified ellison technique, involves shuttling of the IT band underneath the LCL then re-attaching it to its native insertion site at Gerdy’s tubercle. There are several theoretical advantages of the modified ellison that make it an appropriate alternative to the traditional modified lemaire technique.
Purpose: This video overview and case presentation demonstrates the technique for a lateral extra-articular tenodesis via the modified ellison technique.
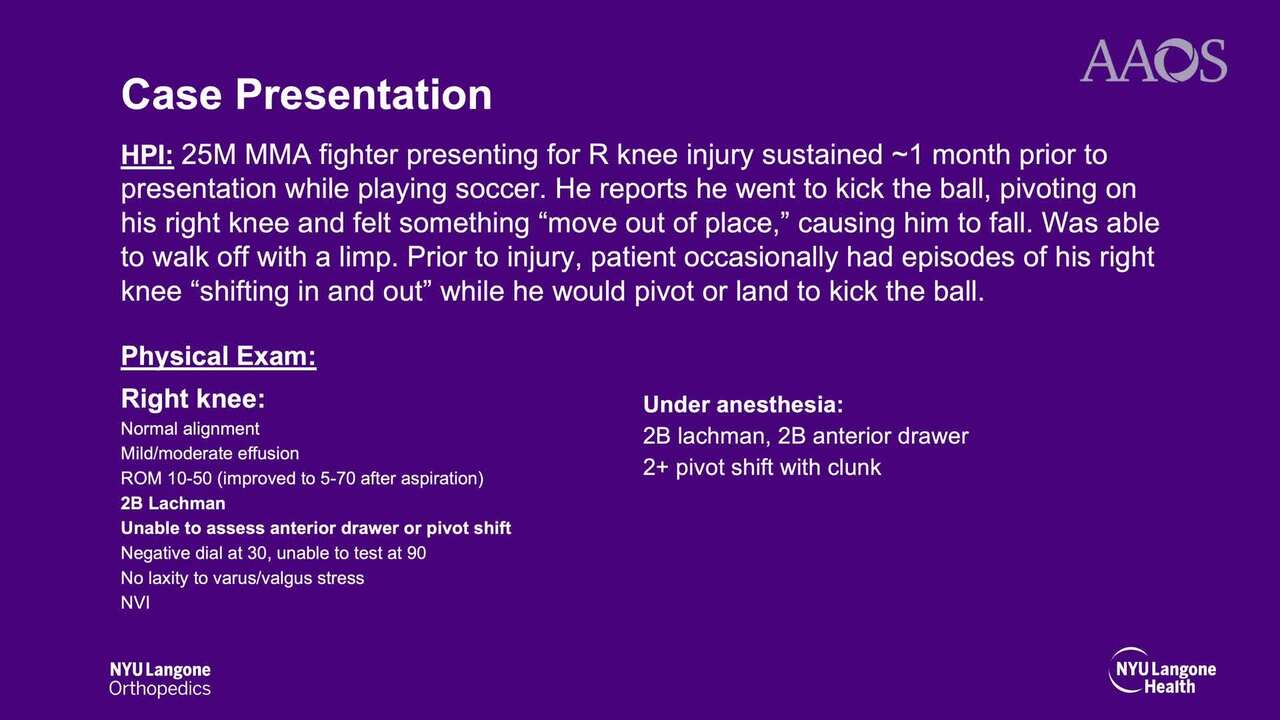
Methods: The anatomy, examination, diagnosis, and treatment options for LET are reviewed. A case of a 25-year-old male with an ACL tear, medial meniscus tear, and medial femoral condyle (MFC) injury is reviewed. This injury occurred while playing soccer and resulted in significant anterolateral rotatory instability as demonstrated by a 2+ pivot shift on exam. After a thorough discussion of risks, benefits and prognosis, the patient elected to proceed with ACL repair with a medial meniscus repair, OATS procedure to the MFC, and LET via a modified ellison technique.
Results: Anterolateral knee laxity was restored intraoperatively. Post-operative clinical outcome showed good restoration of range of motion and stability. The patient was able to return to light jogging and kickboxing within 7 months post-operatively.
Conclusion: There are several theoretical advantages that make the modified ellison a viable technique for lateral extra-articular tenodesis for augmenting an ACL. These include restoration of native knee kinematics, avoidance of femoral ACL tunnels and physes, and lower risk of lateral compartment overrestraint. We believe it is an effective alternative to the more commonly used modified lemaire technique.