ORIF for Comminuted Patella Fracture Using Mini-fragment Plate and Suture Augmentation
Introduction: This video shows the technique for operative fixation of a comminuted patellar fracture using a standard locking mini-fragment plate with suture augmentation. The case is a 75-year-old male who fell directly on his right knee, suffering a highly comminuted fracture of the patella that involves the coronal and sagittal planes, as shown in the preoperative CT scans. The 3D CT reconstruction further confirms the comminuted nature of this injury, as well as the shearing between the articular surface and the anterior cortex, especially distally.
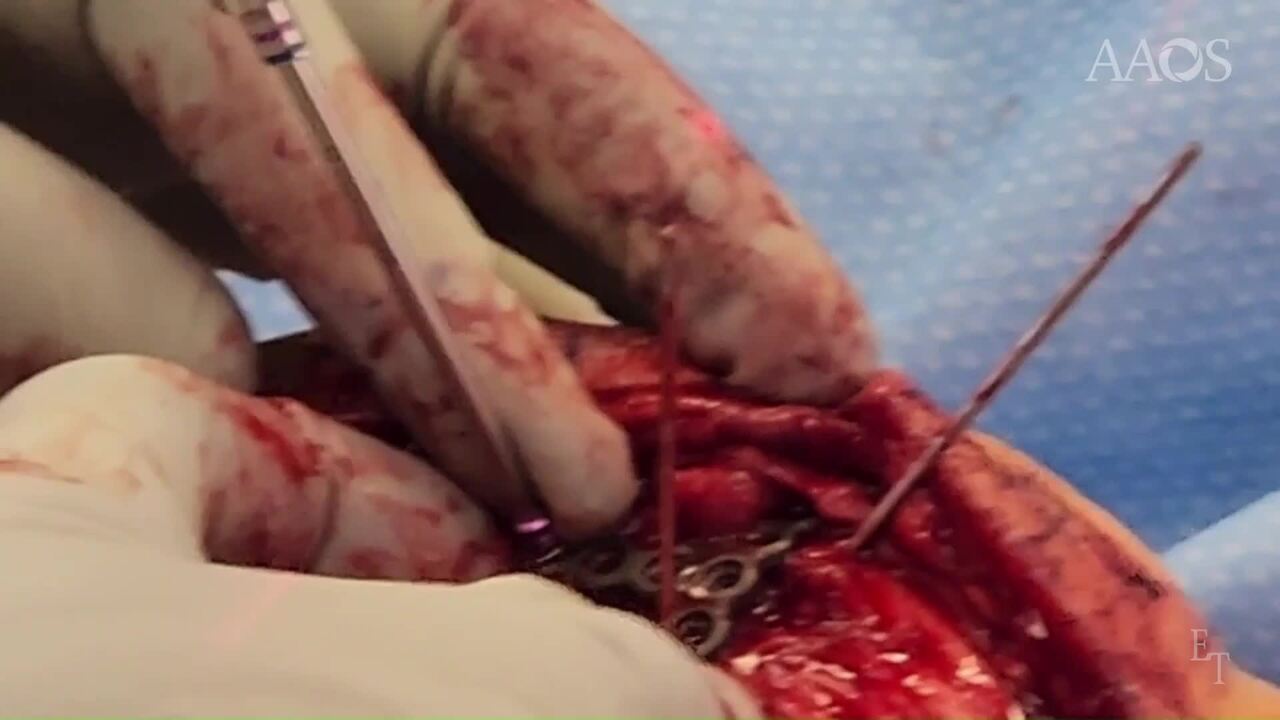
Surgical technique: In the operating room, anatomic landmarks are marked, planning for an anterior longitudinal incision centred directly over the Patella. The skin is incised, and the incision is carried down through deep subcutaneous tissues. The anterior soft tissue is incised to raise medial and lateral flaps to facilitate exposure. Once we get to the level of the fracture, a 15-blade is carefully used to elevate periosteal flaps medially, laterally, proximally, and distally to allow exposure of the highly accommodated distal fragments. The plan at this point is to remove all interposed hematoma and any soft tissues, expecting that reduction of the articular surface will necessitate retraction of the anterior cortical fragments to allow direct manipulation of the articular surface. The fracture is then thoroughly irrigated, and we can begin manipulating each fragment to attempt to reassemble the articular surface. In this case, it was felt that a full parapatellar release of the soft tissues and inverting the Patella itself was not ideal, as it was believed that it would destabilize and de-vascularize multiple fragments. Once we can visualize the articular surface from the fracture, multiple K-wires are placed as joysticks to directly manipulate each fragment. With manipulation of each fragment, reduction clamps are placed from proximal to distal to close any gaps in the lateral plane. Manipulation of the joint surface is directly performed using the joystick to reduce the multiple fracture lines. It's essential that when obtaining lateral views, the knee is both internally and externally rotated to ensure that both the medial and lateral facets are visualized. Once the fracture is reduced, longitudinal K-wires are then placed to provide the initial stabilization. As adequate reduction has been obtained and maintained, a standard mini fragment plate, in this case a long T plate, is cut and contoured to fit the anterior aspect of the Patella. The quadriceps tendon is longitudinally cut to allow the plate to obtain good opposition to the anterior aspect of the proximal Patella. Lateral views confirm ideal placement of the plate for this fracture pattern. And multiple non lock screws are initially placed proximately with great care taken not to penetrate the articular surface. These non-locking screws in general will pull the mini fragment plate into good Bony opposition. Additional non lock screws are placed proximally. Once the plate is fixed to the proximal fragment, any additional fine-tuning of the distal fragments can be performed as the joysticks have remained in place. Before placing any distal locking screws, the longitudinal reduction clamp can be slightly adjusted, and the articular reduction can be fine-tuned. Multiple locking screws then placed distally in the plate, in this case in the medial and lateral fragments independently. Again, internal and external rotation C-arm views are essential to ensure articular reduction. At this point, the options are either placing sutures through the quadriceps tendon into the plate or through the patellar tendon into the plate. Alternately, a braided, high-tensile-strength synthetic suture can be placed in a cerclage fashion. To provide additional stability, the decision about whether the tendons should be sutured to the plate or a cerclage should be used depends on the degree of comminution and the overall stability. In this case, we chose to place a number 5 braided synthetic suture in a cerclage fashion. Once the cerclage and the soft tissues have been completed, it's fully tied, and then anterior soft tissue closure is performed in this case to provide coverage over the plate. This minimizes the risk of soft tissue irritation and hardware irritation. The subcutaneous tissue and skin are then closed in a normal fashion. Monocryl sutures were used to loosely reapproximate the subcutaneous tissue, and 0 proline is placed to close the skin.
Postoperative plan: The plan for this patient, as is standard in our extension mechanism injuries, is for immobilization in a knee immobilizer in full extension without any early range of motion for six weeks. At six weeks, the patient will begin active flexion, passive extension of the knee, and at 12 weeks, we'll begin progressive quadriceps strengthening and resistive aerobic conditioning.