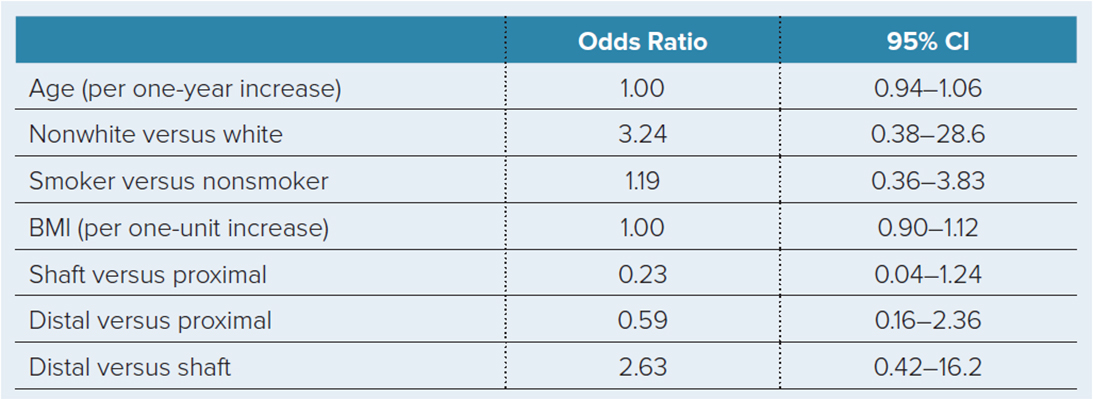
Table 1 Predicted Probabilities of Infection
Courtesy of Christopher Lee, MD
Published 9/3/2021
|
Terry Stanton
A study on low-energy ballistic tibia fractures, to be presented Thursday at 3:30 pm in Ballroom 6B, challenges prior reporting of low complication rates with this injury, suggesting that more vigilant or aggressive treatment strategies may be warranted.
Presenting author Christopher Lee, MD, of UCLA Santa Monica Medical Center—who conducted the study while at R Adams Cowley Shock Trauma Medical Center—told AAOS Now Daily Edition that low-energy ballistic injuries have often been considered comparable to closed injuries, “with very variable management employed in terms of surgical debridement and antibiotic use.”
Dr. Lee explained that his practice has begun “to see a large number of ballistic tibia injuries coming back with surgical-site infections, either aggressively a few weeks post-surgery or as low-grade indolent infections many months later.” Given recent literature showing similar surgical-site infection rates with low-energy ballistic tibia fractures and closed injuries, he and his colleagues sought “to critically evaluate if this were true in the patient population that we were seeing.”
The researchers retrospectively reviewed patients with low-energy ballistic tibia fractures treated at four academic level-one tertiary care referral centers from 2009 until 2019. All patients aged 16 years or older treated with surgical fixation were included.
A total of 197 patients (177 males) with a mean age of 31.9 ± 12.8 years and mean follow-up of 9.2 months (range, 0–121 months) met inclusion criteria. Of the 197 injuries, 135 were shaft fractures, 45 were proximal fractures, and 17 were distal fractures. The overall complication rate was 49 percent (59 of 121). This included:
- 17 patients who developed deep infections (14 percent)
- 33 who developed wound complications (27 percent)
- 24 who developed non-unions (20 percent)
- 11 who developed hardware breakage (9 percent)
- 31 who underwent revision surgery (26 percent)
Deep infections (defined according to the confirmatory criteria by the Fracture Related Infection Consensus Group) occurred in 18 percent (16 of 34 patients) with proximal fractures and 15 percent (11 of 75 patients) with shaft fractures. No patients with distal fractures developed deep infections (Table 1).
“Almost half of all low-energy ballistic tibia fractures developed a complication, with a deep surgical site infection rate of 14 percent,” Dr. Lee said. “We ultimately found a higher-risk complication profile for these gunshot-induced tibia fractures than previously reported.”
The “extremely high complication profile” for those injuries was surprising, he added, as was the high non-union rate of 20 percent.
The clinical takeaway, Dr. Lee said, is that these types of injuries can be challenging. “Surgeons should be wary when encountering these fractures and consider treating these injuries as non–gunshot-induced open tibia fractures,” he said.
For these reasons, he noted, “I have begun to treat these injuries as type II open fractures, including debridement of devitalized bone and thoughtful excision of bullet entry and exit sites [if they are] in particularly precarious locations—especially the anteromedial surface of the tibia. I also find that long-term follow-up, which can be difficult in the trauma patient population, is important, as low-grade indolent infections can persist despite union.”
Overall, he said, he and his colleagues uncovered wide variation in treatment principles with this injury, both in terms of surgical debridement and antibiotic use. “I think future studies to standardize the treatment of these injuries are warranted,” he said.
Addressing limitations of the study, Dr. Lee commented: “Like any retrospective review, selection bias remains, as the type of surgery performed depended on the various surgeons at their respective institutions. Furthermore, low-energy ballistic tibia fractures can represent a wide variation in soft-tissue injury, and this is difficult to account for in a retrospective review.”
Dr. Lee’s coauthors of “Low-energy Ballistic Tibia Fractures: Are Complication Rates Similar to Closed Injuries?” are Dane J. Brodke, MD, MPH; Jamie Engel, MD; Michael G. Schloss, BS; Syed Muhammad R. Zaidi, BS; Robert V. O’Toole, MD; Trevor Gulbrandsen, MD; Matthew Hogue, MD; Justin Badon, MD; Patrick Bergin MD; Seth T. Lirette, PhD; and John Morellato, MD.
Terry Stanton is the senior medical writer for AAOS Now. He can be reached at tstanton@aaos.org.