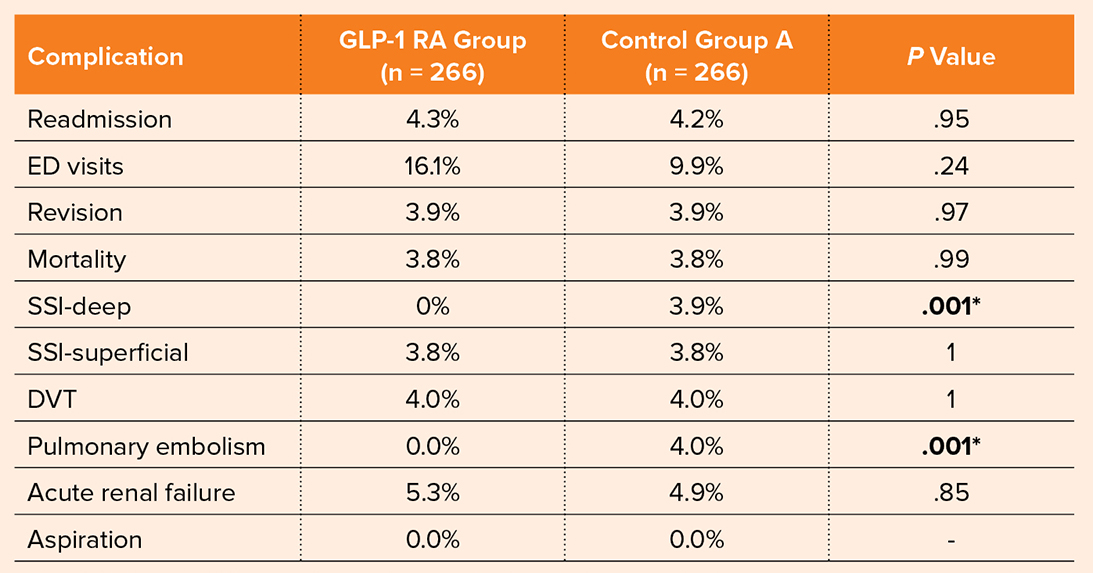
Table 1: Rates of total knee arthroplasty complications between patients who experienced preoperative glucagon-like peptide-1 receptor agonists (GLP-1 RA)-mediated weight loss compared with a control group with a preoperative BMI ≥43 kg/m2 who did not lose weight prior to surgery (control group A)
* denotes statistical significance
SSI, surgical site infection; DVT, deep vein thrombosis; ED, emergency department
* denotes statistical significance
SSI, surgical site infection; DVT, deep vein thrombosis; ED, emergency department
Source: Kagabo W et al. “GLP-1 Receptor Agonist Mediated Weight Loss Improves Outcomes after Total Knee Arthroplasty”
Published 10/19/2025
|
Rebecca Araujo
Researchers from Johns Hopkins Medicine in Baltimore investigated the incidence of complications after total knee arthroplasty (TKA) in patients who experienced preoperative weight loss with the use of glucagon-like peptide-1 receptor agonists (GLP-1 RAs). Their findings were presented as a poster at the AAOS 2025 Annual Meeting by coauthor Whitney Kagabo, MD, orthopaedic surgery resident at Johns Hopkins.
The rising use of GLP-1 RA medications for weight loss and management has been a point of interest in orthopaedic surgery, given the relationship between obesity and joint health. However, “There remains a paucity of literature on the effect of GLP-1 RA–mediated weight loss on outcomes after TKA,” wrote Dr. Kagabo and her colleagues. The research team sought to evaluate the risk profile among patients undergoing TKA who experienced significant preoperative weight loss with GLP-1 RAs.
Table 1: Rates of total knee arthroplasty complications between patients who experienced preoperative glucagon-like peptide-1 receptor agonists (GLP-1 RA)-mediated weight loss compared with a control group with a preoperative BMI ≥43 kg/m2 who did not lose weight prior to surgery (control group A)
* denotes statistical significance
SSI, surgical site infection; DVT, deep vein thrombosis; ED, emergency department
* denotes statistical significance
SSI, surgical site infection; DVT, deep vein thrombosis; ED, emergency department
Source: Kagabo W et al. “GLP-1 Receptor Agonist Mediated Weight Loss Improves Outcomes after Total Knee Arthroplasty”

Table 2: Rates of total knee arthroplasty complications between patients who experienced preoperative glucagon-like peptide-1 receptor agonists (GLP-1 RA)-mediated weight loss compared with a control group with a preoperative BMI ≤40 kg/m2 without GLP-1 RA medication use (control group B)
* denotes statistical significance
SSI, surgical site infection; DVT, deep vein thrombosis; ED, emergency department
* denotes statistical significance
SSI, surgical site infection; DVT, deep vein thrombosis; ED, emergency department
Source: Kagabo W et al. “GLP-1 Receptor Agonist Mediated Weight Loss Improves Outcomes after Total Knee Arthroplasty”
The researchers used the TrinetX research network to identify patients who underwent primary TKA between March 2021 and March 2024 and had achieved a preoperative BMI reduction from ≥43 to ≤40 kg/m2 within one year while prescribed a GLP-1 RA. Patients were propensity-matched 1:1 to two control groups, accounting for demographic factors, laboratory investigations, and comorbidities.
Control group A comprised patients with a preoperative BMI ≥43 kg/m2 who did not lose weight before surgery. Control group B comprised patients with a preoperative BMI ≤40 kg/m2 who were not prescribed a GLP-1 RA prior to TKA. In total, 266 patients in the GLP-1 RA group were matched to control group A, and 268 patients were matched to control group B.
Tables 1 and 2 detail complications among groups. Compared with patients who did not lose weight prior to TKA (group A), the patients in the GLP-1 RA group had a lower risk of deep surgical site infection (0% vs. 3.9%; P = .001) and pulmonary embolism (0% vs. 4%; P = .001). The GLP-1 RA group also had a lower risk of aspiration compared with patients with preoperative BMI ≤40 kg/m2 without GLP-1 RA medication use (group B; 0% vs. 3.7%; P = .001). There were no between-group differences in any other complications. Rates of readmission and emergency department visits were also similar overall.
In conclusion, the authors wrote, “Patients prescribed a GLP-1 RA who underwent significant weight loss prior to TKA had a decreased risk of complications compared to patients who did not lose weight. GLP-1RAs can be an important tool to help patients achieve weight optimization prior to TKA.”
It is critical to note that the above observations may reflect the protective effect of weight loss regardless of weight-loss modality. Further investigations are needed to assess the safety of GLP-1 RA-induced weight loss compared to other strategies for losing weight. Similarly, safe rates of weight loss and comorbid nutritional deficiencies should be explored prior to robust recommendations.
Dr. Kagabo’s coauthors of “GLP-1 receptor agonist mediated weight loss improves outcomes after total knee arthroplasty” are Anirudh Buddhiraju, MBBS; Harpal S. Khanuja, MD, FAAOS; Julius K. Oni, MD, FAAOS; Lucas Nikkel, MD, FAAOS; and Vishal Hegde, MD, FAAOS.
Rebecca Araujo is the managing editor of AAOS Now. She can be reached at raraujo@aaos.org.