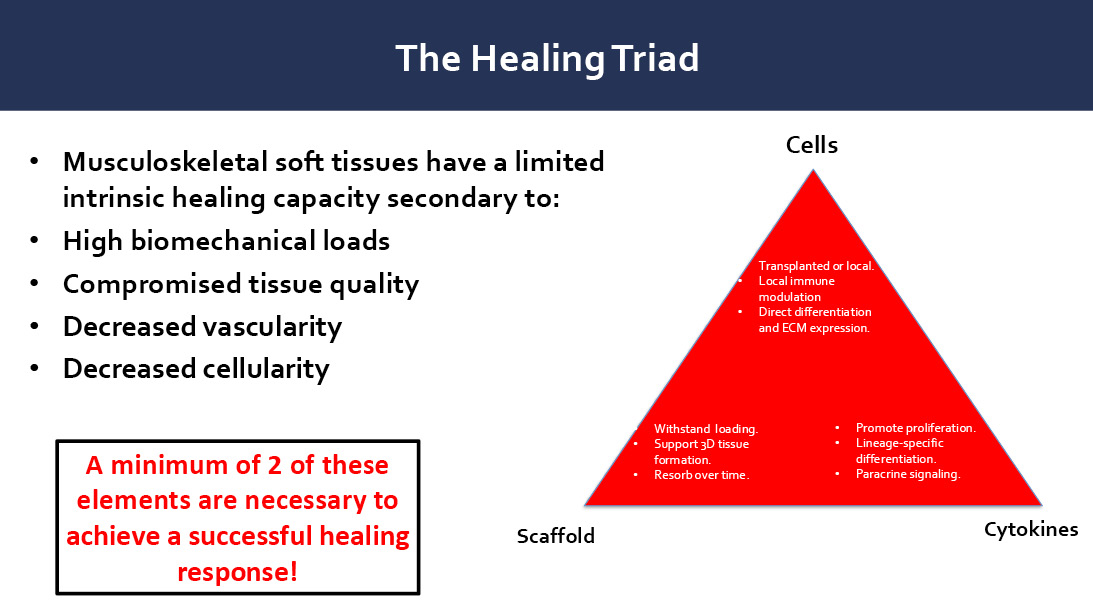
Figure 1: The Healing Triad Caption: Successful musculoskeletal healing depends on three key elements.
Courtesy of Asheesh Bedi, MD, FAAOS
Published 4/24/2026
|
Leah Lawrence
In 2026, there may be no subject that garners more interest in orthopaedics than biologics, according to Asheesh Bedi, MD, FAAOS, executive director and chief of sports medicine at Michigan Medicine.
“There is this benchtop promise, but that has to leap from benchtop to bedside,” Dr. Bedi said. “So the challenge is distinguishing where is the science versus where is the promise?”
During the AAOS 2026 Annual Meeting Instructional Course Lecture “Orthobiologics for Shoulder and Sports Injuries: What is the Evidence?,” Dr. Bedi joined session chair Lewis L. Shi, MD, FAAOS, professor of orthopaedic surgery and rehabilitation medicine at the University of Chicago, and colleagues in tackling that question.
Healing triad
One of the fundamental principles learned from basic science involves the healing triad: cells, scaffold, cytokines (Figure 1).
“In order for us to have healing, particularly in musculoskeletal tissues, we have to have three things tip in our favor,” Dr. Bedi said. “We need responding cells. We need growth factors to influence those cells, and we need some structural tissue.”
The typical healing cascade after surgery or injury involves phases that move from inflammation to proliferation to remodeling and recovery. This is where the potential of platelet-rich plasma (PRP) comes into play.
“PRP has all these different growth factors in it and, theoretically, they are in some physiologic balance or milieu that is important to augment healing,” Dr. Bedi said. “The challenge is that PRP has tremendous heterogeneity, and much of our literature doesn’t report what PRP we deliver.”
In addition, there is not always a distinction between PRP and other autologous solutions, particularly those derived from plasma such as autologous conditioned plasma or autologous protein solution.
“Some of those autologous protein solutions are actually concentrated in other proteins, such as interleukin receptor antagonist protein, [which] has a very potent anti-inflammatory effect, but is, in fact, quite different from PRP,” Dr. Bedi said.
Another fundamental player in this process is stem cells. Although this term is used widely, the two minimal defining features of stem cells are self-renewal and multi-lineage differentiation potential. In 2006, the International Society for Cellular Therapy defined criteria for cells to be considered mesenchymal stem cells: they must be plastic-adherent in standard culture conditions, display specific surface antigens, and demonstrate in vitro differentiation into osteoblasts, adipocytes, and chondroblasts.
“Namely, if they are placed in bone, they become bone; or, if they are placed into connective tissue, they integrate into connective tissue,” Dr. Bedi said. “The challenge is that most of the time when we deliver stem cells in our literature, we don’t actually even prove that they’re stem cells at all.”
Currently in orthopaedics, the most common sources of stem cells are bone marrow aspirate- and adipose-derived stem cells, each with its advantages and disadvantages. “Bone marrow aspirate (BMA) has many nucleated cell populations, and only a small fraction, in fact, meet the criteria of a ‘stem cell,’” Dr. Bedi told AAOS Now. “Accordingly, some of the efficacy of BMA could be attributable to other cells as well as elevated levels of proteins such as Interleukin Receptor Antagonist Program, a well-known inhibitor that modulates inflammation.”
Research into the musculoskeletal applications of these approaches continues.
PRP for rotator cuff repair
Next, Scott A. Rodeo, MD, FAAOS, professor of orthopaedic surgery at Weill Medical College of Cornell University, discussed the role of PRP in rotator cuff tendinopathy and repair.
“Rotator cuff tendinopathy is a painful and dysfunctional shoulder condition traditionally considered as a degenerative pathology,” Dr. Rodeo said. “However, evidence is pointing to immunocompetent cells and activated stromal fibroblasts as the drivers of a non-resolved inflammatory condition in rotator cuff tendinopathy.”
Based on this knowledge, it is thought that cell therapy may have a role in treating tendon disease, and there is some evidence to support the claim.
One study from 2021 followed 99 patients with rotator cuff tendinopathy (RCT) and partial-thickness rotator cuff tears (PTRCTs) who received either ultrasound-guided PRP or corticosteroid injection. Patients experienced clinical improvement in pain and patient-reported outcomes after both, but those who received PRP had superior improvement in pain and function at short-term follow-up.
Another study from researchers in Argentina included patients with RCT or PTRCT and treated them with leukocyte-rich PRP injections. Here, the injections improved shoulder function, pain, and sleep disturbances in most patients with RCT, maintained up to 12 months; however, these benefits were not as substantial in the patients with PTRCT.
Evidence also varies for PRP in rotator cuff repair. A meta-analysis published in 2020 that focused on level 1 randomized controlled trials indicated that clinical outcomes were positively affected and long-term retear was significantly reduced among patients who received PRP. Another meta-analysis compared the use of PRP with corticosteroids for rotator cuff injuries and found that corticosteroids had better short-term efficacy, but PRP was more beneficial long-term. Finally, a more recent meta-analysis comparing PRP plus surgery to surgery alone showed a significant decrease in retear rates with the addition of PRP.
Dr. Rodeo also discussed the current evidence on the use of cell therapy for rotator cuff repair, a strategy that he said is promising for improvement in structural healing, but requires further study.
Biologic augmentation techniques
Finally, Jason L. Koh, MD, MBA, FAAOS, an orthopaedic surgeon specializing in sports medicine at Endeavor Health, gave an overview of biological augmentation using bone marrow.
One of the techniques he discussed was the “Crimson Duvet,” as described by Synder and Burns, which involves creating microfractures in the tuberosity to release bone marrow.
“The initial idea was to make perforations lateral to the area of repair, and they found in their studies that they had a retear rate of only 8%,” said Dr. Koh, adding that these findings are backed up by several animal studies.
“Other authors have proved that multiple channeling can improve the structural integrity of rotator cuff repair with significant improvements in terms of healing rate and decreased retear,” Dr. Koh said.
More recently, studies have looked at this prospectively in randomized trials. A meta-analysis of some of these studies did not support bone marrow stimulation to improve retear rates, but there was a trend showing that smaller, 1-mm needle holes caused less disruption and may result in improved tendon healing rate. In contrast, another meta-analysis demonstrated significantly lower retear rate with marrow stimulation, with retear rates as low as 17.5%.
“So in general, if you want to try to bring those wonderful cells and factors to an area that has very limited blood supply and limited ability to heal, this [local bone marrow stimulation] is one technique,” Dr. Koh said.
Leah Lawrence is a freelance medical writer for AAOS Now.
References
- Kwong CA, Woodmass JM, Gusnowski EM, et al. Platelet-rich plasma in patients with partial-thickness rotator cuff tears or tendinopathy leads to significantly improved short-term pain relief and function compared with corticosteroid injection: a double-blind randomized controlled trial. Arthroscopy. 2021;37(2):510-517.
- Rossi LA, Piuzzi N, Tanoira I, et al. Subacromial platelet-rich plasma injections produce significantly worse improvement in functional outcomes in patients with partial supraspinatus tears than in patients with isolated tendinopathy. Arthroscopy. 2023;39(9):2000-2008.
- Chen X, Jones IA, Togashi R, Park C, Vangsness CT. Use of platelet-rich plasma for the improvement of pain and function in rotator cuff tears: a systematic review and meta-analysis with bias assessment. Am J Sports Med. 2020;48(8):2028-2041.
- Peng Y, Li F, Ding Y, et al. Comparison of the effects of platelet-rich plasma and corticosteroid injection in rotator cuff disease treatment: a systematic review and meta-analysis. J Shoulder Elbow Surg. 2023;32(6):1303-1313.
- Trantos IA, Vasiliadis ES, Giannoulis FS, et al. The effect of PRP augmentation of arthroscopic repairs of shoulder rotator cuff tears on postoperative clinical scores and retear rates: a systematic review and meta-analysis. J Clin Med. 2023;12(2):581.
- Snyder SJ, Burns JP. Rotator cuff healing and the bone marrow “crimson duvet” from clinical observations to science. Techniques in Shoulder & Elbow Surgery. 2009;10(4):130-137.
- Hurley ET, Crook BS, Danilkowicz RM, et al. Bone marrow stimulation for arthroscopic rotator cuff repair: a meta-analysis of randomized controlled trials. Am J Sports Med. 2024;52(12):3167-3172.
- Yang G, Li S, Jiang C, Zhang H, Lu Y. The role of bone marrow stimulation in rotator cuff repair: a systematic review and meta-analysis. J Exp Orthop. 2023;15;10(1):27.