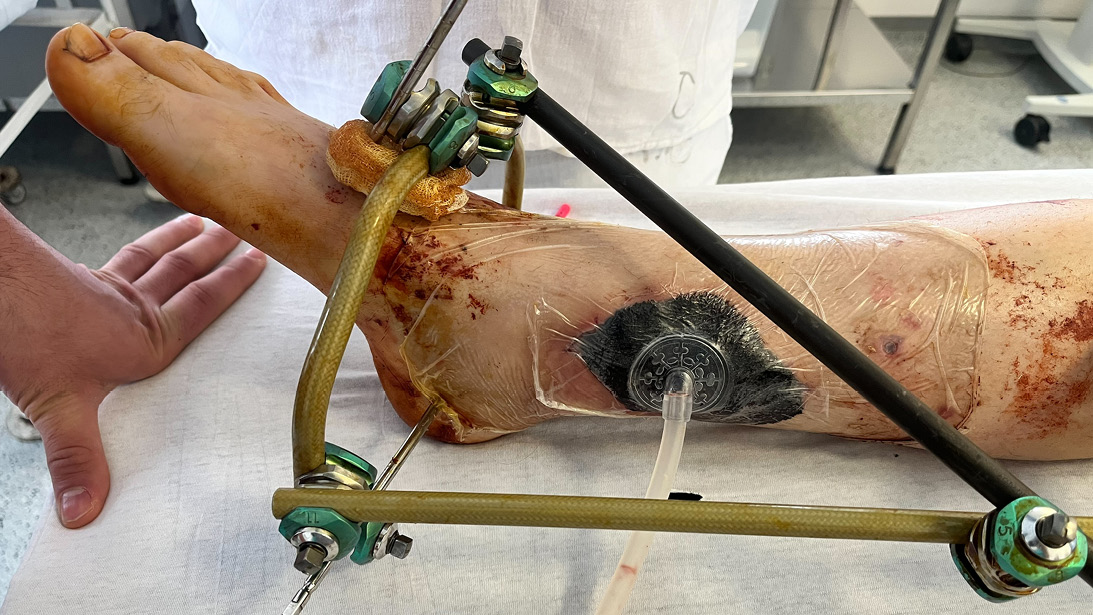
Figure 1: A patient with severe tibial trauma from a drone attack with an open distal third tibial fracture
Courtesy of Douglas W. Lundy, MD, MBA, FACS, FAAOS
Published 4/25/2026
|
Douglas W. Lundy, MD, MBA, FAAOS
In October 2005, I traveled to Prishtina, Kosovo, to participate in my second mission trip. Hearing stories from Kosovars and seeing the scars of war-related devastation had a profound impact on my worldview. That perception was relatively static throughout the 31 subsequent trips I took to the developing world until I recently traveled with Roman Hayda, MD, FAAOS, to Dnipro, Ukraine.
Dr. Hayda is currently the chief of orthopaedic trauma surgery at Brown University, having retired from the US Army as a colonel. Dr. Hayda grew up in a Ukrainian household and lived in a Ukrainian community in Michigan. He speaks fluent Ukrainian and has a tremendous passion to help people in this war-torn country. When he asked if I could accompany him on one of his many journeys to the country, how could I possibly say no? (Read more about my trip in “A problem from hell: The Russia-Ukraine war” from the March issue of AAOS Now.)
Figure 1: A patient with severe tibial trauma from a drone attack with an open distal third tibial fracture
Courtesy of Douglas W. Lundy, MD, MBA, FACS, FAAOS

Figure 2: The patient (in prone position) after placement of an antibiotic spacer
Courtesy of Douglas W. Lundy, MD, MBA, FACS, FAAOS

Figure 3: The patient after application of ring fixation, Masquelet technique, and reverse sural artery rotational flap coverage
Courtesy of Douglas W. Lundy, MD, MBA, FACS, FAAOS
Admittedly, once I learned how dangerous this trip could be, I second-guessed this decision far more than I had questioned any previous trip. The sending agency required us to download apps to our phones that would alert us in case of an air raid and help rescuers find us (or at least our phones!) if we were hurt. My phone started alerting me immediately, well before I even left the United States! The frequency and intensity of these alerts caused me a measured amount of concern.
Through Roman’s contacts, we were invited to work at two separate trauma hospitals in Dnipro, Ukraine, which is approximately 60 miles from the front, helping the courageous orthopaedic surgeons with their suffocating workload. What we found left me amazed.
Ukraine is a country of only 32.8 million people (2025 estimate) that finds itself at war with a country more than four times its size. Mandatory conscription of all Ukrainian males between 25 and 60 years of age underscores the monolithic challenge facing Ukraine to defend its sovereignty, independence, and freedom. Sadly, such intense combat action results in violent death or severe injury to many of these soldiers, straining the national trauma network.
The sobering reality of Ukraine’s plight was underscored the very first night, as I stared at the ceiling from jet lag. At 2 a.m., the air attack alarms sounded on my phone, notifying me that intermediate-range ballistic missiles were inbound to the city of Dnipro. These alarms are so frequent that the Ukrainian people almost seem to take them in stride. I listened carefully to see if guests were making their way to the shelter, but hearing no movement, I foolishly decided to wait in my room. Shortly, I heard missiles flying overhead and the subsequent impact on a heating facility just miles from our hotel. It was harder to sleep after that.
Mechnikov Hospital is the closest large trauma center to the front lines, and, not surprisingly, it receives high volumes of trauma patients. The advent of drone warfare has made medical evacuation from the front incredibly hazardous, and it is not uncommon for injured soldiers to wait a day or more to be evacuated from the trenches. Due to air combat superiority, the United States was able to medevac injured soldiers relatively efficiently from battle in Afghanistan and Iraq, but that capability is nearly impossible in Ukraine, as aerial drones from both sides quickly strike medevac helicopters and ground transport.
As a result, we encountered multiple cases of patients presenting with severe open extremity injuries, often due to mine blasts, drone attacks, or direct combat trauma. Not surprisingly, many of these soldiers sustained varying degrees of frostbite as they were waiting to be evacuated from the action. Extremity tourniquets had been applied to many of these soldiers, resulting in irreversible ischemia, unfortunately requiring amputation.
Mechnikov Hospital provides immediate stabilization and initial care to soldiers but must transfer these patients further west for definitive treatment to make room for the next wave of traumatized patients. Civilians injured in action remained at Mechnikov for reconstruction, but this surgery was often delayed due to the oppressive volume of acutely injured patients requiring urgent surgical attention.
The Ukrainian State Institute of Medical and Social Problems of Disability in Dnipro serves as one of the facilities that can provide definitive treatment, and we assisted the Ukrainian surgeons in working through these extremely complex injury patterns. Tension wire circular ring external fixation and rotation soft tissue flap coverage technique became a mainstay of injury reconstruction. Patients presented with massive bone and soft tissue defects that would strain the imagination and resources of any trauma center in the world. Masquelet bone grafting and distraction osteogenesis techniques are employed daily to restore limb function.
All of the instruments and implants we used were from donated sources, and the variety of constructs available was limited. By applying sound trauma principles and making the most of the resources available, we were able to deliver the highest standard of care under these conditions. Throughout the entire experience, the administration, surgeons, and staff of these hospitals remained the most gracious and appreciative healthcare workers I have ever encountered.
The ever-present threat of attack looms in the Ukrainian mindset. Several months ago, one of the neurosurgeons at Mechnikov was performing a craniotomy on an injured soldier when a Russian ballistic missile struck the wall of the operating room, destroying the operating theater. The neurosurgeon, who happened to be the son of the Department Chair of Neurosurgery, narrowly escaped with his life. Considering the incredible resolve of these professionals, it was not surprising that they quickly rebuilt the operating rooms and continued their mission.
When Dr. Hayda first talked with me about this work, I commented that the Ukrainian people were “his people” due to his heritage and cultural upbringing. He quickly corrected me that the Ukrainian people are “our people,” and after my experience in Dnipro, I could not agree more. There are many ways we can support the medical efforts in Ukraine, and I encourage the readership to do so.
Roman A. Hayda, MD, FAAOS, contributed to this article.
Douglas W. Lundy, MD, MBA, FACS, FAAOS, is chair of orthopaedic surgery and chief of orthopaedic trauma surgery at St. Luke’s University Health Network in Bethlehem, Pennsylvania. He is also the deputy editor of AAOS Now and a member of the AAOS Now Editorial Board.