
Figure 1: Caption: Wide awake, local anesthesia, no-tourniquet (WALANT) surgery has expanded hand surgery into office-based settings for routine procedures.
Published 4/24/2026
|
Sam Moghtaderi, MD, FAAOS
Five years ago, a 70-year-old mechanic with a 60-degree composite small finger due to Dupuytren’s contracture would have been scheduled for surgery in the operating room, likely with general anesthesia or sedation. This would come with a preoperative visit to the lab for bloodwork, an overnight fast, and a family member taking a day off work to accompany the patient. Today, in select practices around the country, that same patient walks into the clinic without prior lab work or fasting, has the same open fasciectomy procedure, and takes public transit home a few hours later. This is not fiction; rather, it is one example of the frontiers of in-office hand surgery in 2026.
Wide awake, local anesthesia, no-tourniquet (WALANT) surgery has been transformative in hand surgery over the last decade. Technique refinements now allow for awake surgery with reliable hemostasis and patient comfort. Hand surgeons have widely adopted WALANT in the operating room and, increasingly, in the clinic setting for routine cases such as trigger finger release, carpal tunnel release, and simple mass excisions. In-office surgery provides ease of scheduling, greater efficiency, and significant improvements to the patient experience.
Figure 1: Caption: Wide awake, local anesthesia, no-tourniquet (WALANT) surgery has expanded hand surgery into office-based settings for routine procedures.
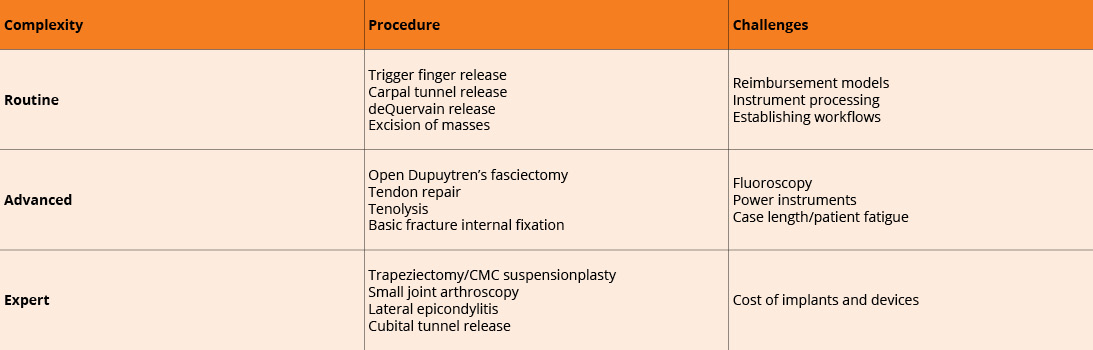
Table 1. A broad range of cases can be considered for in-office hand surgery.
Courtesy of Sam Moghtaderi, MD, FAAOS
As experience with in-office surgery has grown, the range of what is possible in the clinic setting has been expanding. Yet challenges remain that limit adoption. The appropriateness of a case for clinic is no longer constrained by anesthesia technique, but rather the surgeon’s experience and the practice environment. Surgery in the office requires having a workflow for managing sterile instruments, which can be processed with small countertop autoclave devices run by office staff. The limited number of instruments required for carpal tunnel surgery and similar procedures is very practical for clinic staff to manage without the support of a full hospital sterile processing department, but sterilizing more advanced equipment, such as power instruments and fluoroscopy, may prove limiting. Procedure length must also be considered, as patients realistically can tolerate about 60 to 90 minutes lying on an office stretcher or in a reclining chair before positioning becomes fatiguing for them.
Still, with the appropriate surgeon experience and in the right practice environment, some have expanded the scope of in-office surgery beyond the simplest of cases. Increasingly common are the exploration of simple wounds, tendon repairs, open fasciectomy for Dupuytren’s disease, straightforward fracture fixation with Kirschner wires, and procedures that benefit from the patient’s active participation, such as tenolysis or tendon repairs and transfers. Less common in the clinic setting but still possible with more advanced WALANT technique are bony procedures such as trapeziectomy or carpometacarpal (CMC) arthroplasty of the thumb. In-office small joint arthroscopy is also emerging, with newer self-contained units on the market. As clinicians become increasingly comfortable providing adequate local anesthesia, soft tissue procedures about the elbow, such as cubital tunnel release and open treatment of lateral epicondylitis, can be considered as well.
Reimbursement challenges ease with CMS changes
Even though advancing expertise with WALANT has allowed hand surgeons to perform an increasing proportion of their procedures with the patient awake, one of the biggest limiting factors that prevents transition from the operating room to the office has been the reimbursement model in the United States. Unlike the hospital outpatient or ambulatory surgery center, the clinic is considered a “non-facility” site of service in most practice settings, with no provision to charge a separate facility fee to cover practice expenses. While in-office surgery has been shown to greatly reduce waste and total cost to the healthcare system, minimal costs remain that must be accounted for in any sustainable financial model.
In 2026, a significant change in the Centers for Medicare & Medicaid Services (CMS) Physician Fee Schedule has made the challenging payment landscape somewhat more favorable for this transition. While the 2026 CMS changes decrease payments across the board for all surgical services due to new efficiency-based adjustments, an additional decrease to practice expense reimbursement has been applied only to procedures in hospital facility settings. CMS has explicitly exempted non-facility settings from this practice expense cut, incentivizing a transition from the OR to clinic settings. The net result is that in 2026 and beyond, professional fees for common hand procedures in non-facility settings may be modestly higher than for those same procedures performed in the operating room. While generally representing only a small increase in the compensation for in-office surgery, the relative decline of payments for cases performed in the OR means transitioning appropriate cases to clinics will minimize the impact of the 2026 CMS cuts.
The convergence of increasing WALANT expertise and improved payment incentives creates real opportunity for expansion of in-office hand surgery in 2026. Yet this is not a call to rush every case out of the OR. Practices that have not already done so now have a more straightforward path to transitioning routine hand surgery cases to an in-office setting, but only after investing time in developing appropriate workflows, staff training, and sustainable practice models.
When done well, in-office surgery delivers benefits to all stakeholders — giving patients convenient, efficient, high-quality care while creating sustainable practice models and significantly decreasing waste and overall cost to the healthcare system. These benefits lay the groundwork for continuing to expand the spectrum of procedures performed in the office setting as surgeon experience and practice capabilities advance.
Sam Moghtaderi, MD, FAAOS, is assistant professor of orthopaedic surgery and residency program director at the George Washington University School of Medicine and Health Sciences in Washington, DC.