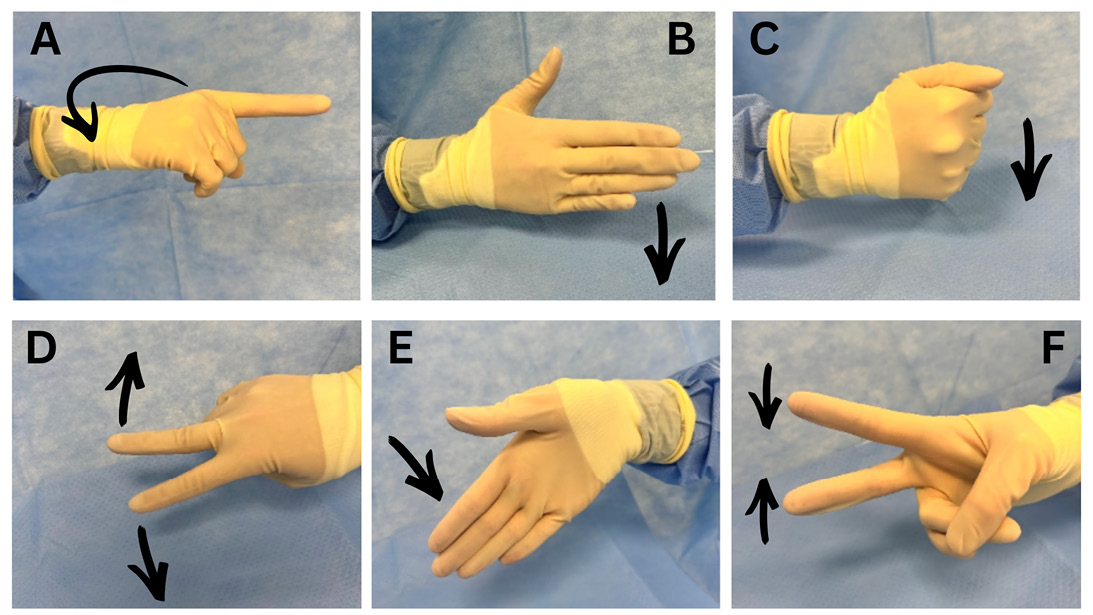
Figure 1 Caption: West Virginia University developed a set of hand signals to enable clear and discreet communication during WALANT procedures. A: “Start.” The index finger is extended while the fist is clenched and the wrist is supinated. B: “Stop.” The ulnar border of a flat hand is placed against the operating table. C: “Help.” A clenched fist is placed against the operating table. D: “Dissect.” The index and middle fingers are extended and spread while the remaining fingers remain flexed. E: “Cut with scalpel.” A flat hand is placed in the air with the ulnar border toward the table and the wrist is deviated ulnarly. F: “Cut with scissors.” The index and middle fingers are extended and abducted toward one another while the ring and small fingers are flexed with the thumb flexed over them.
Published 4/17/2026
|
Kaley Haney, MD; Nathaniel Williams, MD; Kenneth Sabacinski, MD; Shafic Sraj, MD; John S. Taras, MD
Wide-awake local anesthesia with no tourniquet (WALANT) has become a cornerstone of modern orthopaedic surgery and hand surgery in particular. As surgeons balance patient comfort, efficient team communication, and the growing demands of resident and fellow education, the need for nonverbal communication in the procedure room has become more apparent.
Procedure rooms are increasingly used as cost-effective and efficient settings across multiple medical practices, driving a push to perform more procedures outside traditional surgical centers and hospitals. Over the past decade, accelerated adoption of WALANT has allowed many common procedures to be performed safely outside the operating room. Numerous studies have demonstrated that WALANT procedures result in infection rates comparable to those seen in the operating room, decreased time to surgery, high patient satisfaction, and substantial cost savings. As a result, procedures such as carpal tunnel release, trigger finger release, mass excision, and treatment of Dupuytren’s contracture are now frequently — and, in some practices, almost exclusively — performed in clinic-based procedure rooms.
Figure 1 Caption: West Virginia University developed a set of hand signals to enable clear and discreet communication during WALANT procedures. A: “Start.” The index finger is extended while the fist is clenched and the wrist is supinated. B: “Stop.” The ulnar border of a flat hand is placed against the operating table. C: “Help.” A clenched fist is placed against the operating table. D: “Dissect.” The index and middle fingers are extended and spread while the remaining fingers remain flexed. E: “Cut with scalpel.” A flat hand is placed in the air with the ulnar border toward the table and the wrist is deviated ulnarly. F: “Cut with scissors.” The index and middle fingers are extended and abducted toward one another while the ring and small fingers are flexed with the thumb flexed over them.
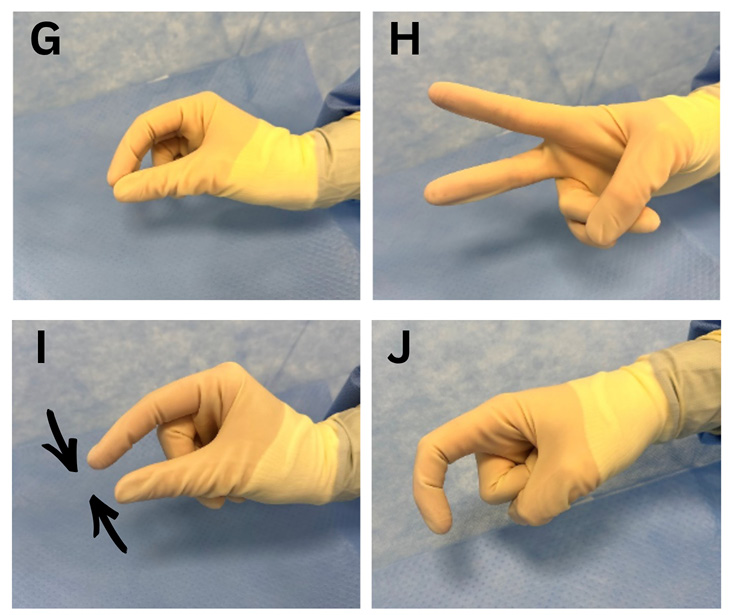
Figure 2 West Virginia University’s hand signals help surgeons communicate during awake, in-office surgery. G: “Scalpel.” The index finger and thumb are held together as if grasping a scalpel. H: “Scissors.” The index and middle fingers are extended and held abducted away from one another while the ring and small fingers are flexed with the thumb flexed over them. I: “Forceps.” The index finger and thumb are pinched toward one another while the remaining fingers remain flexed. J: “Suture.” The index finger is curled while the other digits remain in a fist.
As the clinic-based procedure room setting becomes central to many orthopaedic practices across the country, it becomes necessary to incorporate office-based surgery into resident and fellow education.
While WALANT surgery offers clear advantages for patients, surgeons, and health systems, its popularity has introduced new challenges related to intraoperative communication, especiallyregarding surgical education. During WALANT procedures, patients remain fully awake and coherent, requiring surgeons and staff to be mindful not only of what is communicated but also how it is communicated. Routine surgical language — terms such as “cut,” “dissect,” or even the names of common instruments — may be alarming to patients and can disrupt the calm environment essential to the completion of a successful procedure. Even whispered conversations between surgical team members may increase patient concern and undermine confidence in the surgeon or procedure.
As graduated autonomy in surgical programs continues, it becomes essential that residents and fellows participate in WALANT surgeries prior to graduation, not only as an assistant but, eventually, as the primary surgeon. Because patients are awake, there can be difficulty with verbal corrections and guidance from an attending to a resident surgeon. Many foundational hand procedures that are critical (and required) components of resident and fellow education are now performed almost exclusively in the procedure room setting. Historically, these cases were conducted in the operating room, where verbal instruction, step-by-step guidance, and (at times) immediate correction were integral to surgical training and patient safety.
The transition to wide-awake procedures places an additional burden on attending surgeons to modify their teaching style, often limiting verbal instruction to preserve patient comfort. Without an alternative strategy, resident and fellow education may be significantly compromised, or trainees may be excluded from invaluable learning experiences. These necessary changes can be achieved through a combination of altering communication amongst surgical team members and providing patients with opportunities for entertainment that serve as alternatives to ongoing activities on the other side of the drapes.
The use of lesser-known terms such as “Bard” in place of scalpel, hand gestures to direct resident maneuvers, and even TV or music access have become important practices at West Virginia University to continue resident education and growth while alleviating patient stress. Informal hand gestures have long existed in surgical practice; however, specific gestures have been developed and described specifically for WALANT procedures and for addressing the unique educational challenges posed by the procedure room setting. At West Virginia University, a set of hand signals was developed to enable clear and discreet communication during WALANT procedures. Four fellowship-trained hand surgeons were surveyed to identify the most essential actions and instrument requests requiring intraoperative communication, particularly when supervising resident surgeons. Six procedural actions and four commonly used instruments were identified as warranting hand signals. Ten hand signals were developed (Figures 1, 2), all designed to be intuitive, reproducible, and performed with one hand, allowing seamless integration into the routine workflow while minimizing cognitive burden for surgeons and trainees.
Patient entertainment can take many forms. It can be as simple as patients bringing their own devices, such as music players or streaming services. Other options include providing live TV in the room or providing immersive experiences using virtual reality (VR) devices. TVs and VR devices also allow patient education if the practice chooses to communicate mandatory perioperative instructions through the media provided. It could also be as simple as a guided conversation with the circulating team member.
Awake surgery offers the experience of many conversations, some funny and interesting and some bordering on “sharing too much info.” The entertainment serves as a distraction and can be very helpful to patients who may be hesitant or anxious yet still choose to pursue in-office awake surgery. The choice of what is offered is partly dictated by surgeon preference. Some surgeons prefer highly distracted patients and thus encourage VR devices and earphones, whereas others prefer uninterrupted communication with patients and consequently favor ambient entertainment such as in-room TV or music and conversations.
As WALANT continues to reshape orthopedic surgery, education in this unique surgical practice should become a building block for all residents. Communication strategies for WALANT surgeries must evolve in tandem with this education. A hand signal system and the use of alternative words for surgical tools are simple and reproducible interventions with the potential to improve patient experience, optimize operative efficiency, and support the educational mission of orthopaedic training programs. Adopting similar communications may further enhance the safety, effectiveness, sustainability, and educational value of wide-awake hand surgery, especially at teaching facilities.
Kaley Haney, MD, is a PGY-2 resident in the Department of Orthopaedics at West Virginia University, Morgantown, West Virginia.
Nathaniel Williams, MD, is an adult reconstruction fellow at Vanderbilt University, Nashville, Tennessee.
Kenneth Sabacinski, MD, is an adult reconstruction fellow at the Beth Israel Deaconess Medical Center, Boston.
Shafic Sraj, MD, MBA, FAAOS, is the director of orthopaedic surgery at the Valley Health Center for Orthopedic Excellence in Winchester, Virginia. He specializes in hand and upper extremity surgery and wide awake and in-office surgery and is an adjunct professor of orthopaedics at West Virginia University.
John S. Taras, MD, FAAOS, is professor, chief of hand and upper extremity surgery in the Department of Orthopaedics at West Virginia University.