Published 2/27/2026
|
Alyssa Barré, MD; Vince Prusick, MD
Perioperative care for adolescent idiopathic scoliosis (AIS) has shifted from individualized, surgeon-dependent practice toward standardized recovery pathways. Enhanced recovery after surgery (ERAS) protocols have accelerated this transition by emphasizing consistency, reproducibility, and coordinated care across disciplines. Within these pathways, perioperative pain management is a central driver of earlier mobilization, predictable length of stay, and safe discharge.
As length of stay has shortened, the goals of postoperative analgesia have evolved. Rather than eliminating pain entirely, contemporary pain management strategies are designed to provide reliable, function-supporting analgesia that enables early ambulation, participation in physical therapy, and transition to oral medications on a defined timeline. The University of Kentucky and Shriners Children's Lexington have together successfully employed a standard ERAS protocol with an embedded pain strategy over the last several years and have seen a steep decline in length of stay after posterior spinal fusions for AIS, with about half of patients leaving the hospital on postoperative day one.
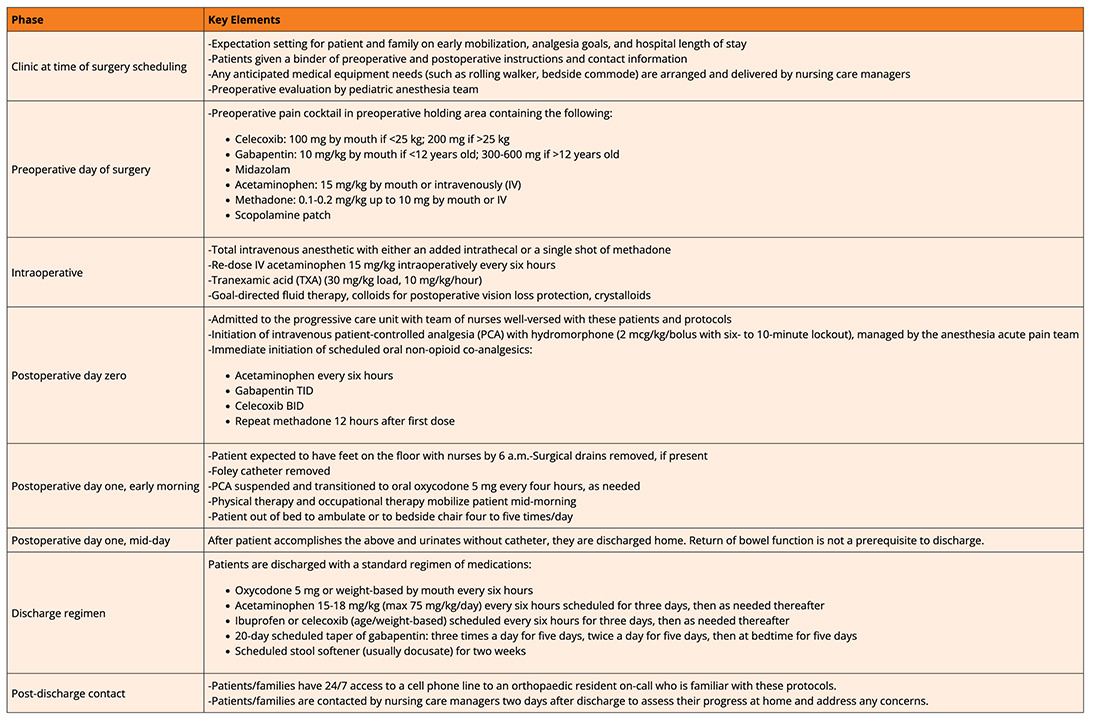
Table 1: University of Kentucky and Shriners Children’s Lexington’s institutional protocol for perioperative management of patients undergoing posterior spinal fusion for adolescent idiopathic scoliosis (AIS). Note that medications and dosages are general guidelines and can change based on patient age, weight, medical conditions, allergies, etc.
Standardized multimodal pain management
Modern ERAS pathways approach perioperative pain management as a standardized process rather than an individualized response to postoperative discomfort. Historically, opioid-dominant regimens tailored to surgeon preference provided effective analgesia but introduced variability and side effects that delayed mobilization and prolonged hospitalization.
Within contemporary pathways, multimodal analgesia serves as the primary mechanism for standardization. By combining medications with complementary mechanisms of action, effective pain control can be achieved while limiting reliance on high-dose opioids. Scheduled non-opioid medications establish a stable analgesic baseline, with opioids reserved for breakthrough pain. This structure reduces pain variability, minimizes opioid-related side effects, and supports earlier mobilization.
Equally important, consistent dosing schedules and predefined transition points, particularly the planned early transition from intravenous to oral analgesia, allow recovery milestones to be anticipated rather than negotiated. For surgeons, this predictability is essential when discharge planning begins before surgery rather than after.
A team approach is essential
Effective perioperative pain management within ERAS pathways depends on coordinated, multidisciplinary execution rather than isolated decision making. Pain control, mobilization, and discharge planning are shared objectives that require consistent communication across the perioperative teams. When clinic, nursing, anesthesia, pain, therapy, and surgical teams operate within a common framework, analgesic strategies are applied consistently and recovery milestones are reinforced, allowing recovery to progress according to plan.
ERAS protocol results in increased next-day discharge without unplanned return to care
To translate these principles into practice, the University of Kentucky and Shriners Children's Lexington employ a standardized, multidisciplinary perioperative pain management strategy integrated into an ERAS protocol (Table 1). The pathway is designed around predefined transitions, with expectations for analgesia, mobilization, and discharge established at the time of surgical scheduling. Pain management is initiated preoperatively, reinforced intraoperatively, and structured postoperatively to support early mobilization and planned transition from intravenous to oral analgesia on postoperative day one. Functional milestones, rather than pain scores alone, guide progression through the pathway and determine discharge readiness.
Using this approach, next-day discharge has been safely achieved in a substantial proportion of patients without an increase in emergency department visits or hospital readmissions. Importantly, success is attributed to pathway consistency and involvement of the full team of providers, rather than any single analgesic agent, and is reliant on care and education that starts prior to surgery and extends after leaving the hospital.
Conclusion
For surgeons implementing or refining ERAS pathways for AIS, perioperative pain management should be approached as an operational tool that directly influences recovery timelines. Analgesic strategies must be intentionally aligned with functional milestones and executed consistently across the care continuum.
As perioperative care continues to evolve, pain management will remain a central driver of successful AIS recovery. When approached as a systems-level tool rather than an isolated intervention, analgesia enables consistent recovery, early mobilization, and safe discharge.
Alyssa Barré, MD, is an orthopaedic surgery resident at the University of Kentucky in Lexington, Kentucky.
Vince Prusick, MD, is a pediatric orthopaedic surgeon and associate professor of orthopaedic surgery at the University of Kentucky and Shriners Children's Lexington in Lexington, Kentucky.
References
- Kirk AM, Barré AM, Prusick VW, Conley C, Muchow RD. Is next-day discharge safe after posterior spinal fusion for adolescent idiopathic scoliosis? J Pediatr Orthop. 2025 Jan 1;45(1):e37-e42. doi:10.1097/BPO.0000000000002792. Epub 2024 Aug 22. PMID: 39171367.
- Weintraub MJ, Gupta A, Kaushal NK, McIntosh AL, Hasley BP, Sardar ZM; SRS Safety And Value Committee. State of the art review: enhanced recovery after surgery (ERAS) protocols in adolescent idiopathic scoliosis. Spine Deform. 2025 Dec 2. doi:10.1007/s43390-025-01241-6. Epub ahead of print. PMID: 41331229.
- Creyf P, Parisi N, Munting S, Caudron M, Rossillon R, Detrembleur C, Munting E. Enhanced recovery after adolescent idiopathic scoliosis surgery care pathway: Perioperative strategy to improve outcome. Brain Spine. 2024 Aug 31;4:103326. doi:10.1016/j.bas.2024.103326. PMID: 39381755; PMCID: PMC11458952.