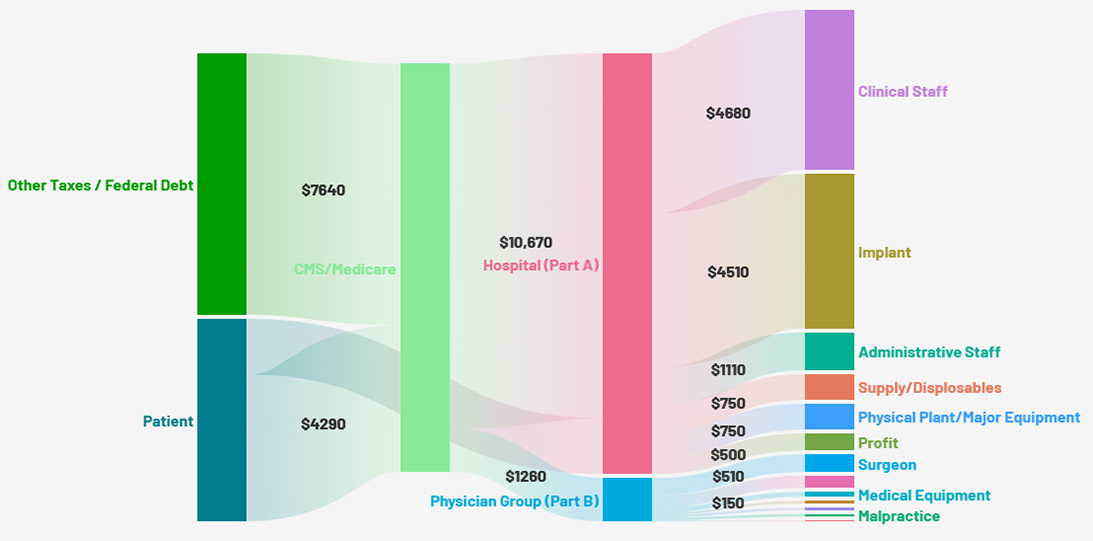
Figure 1: A schematic representation of the major financial flows for a hip replacement.
Courtesy of Eric Swart MD, FAAOS
Published 6/22/2026
|
Eric Swart, MD, FAAOS; Elizabeth Duckworth, MD, MBA; Abner Ward, MD, FAAOS
Physicians are familiar with how their daily work and decisions affect their personal reimbursement and finances, but many lack a broader understanding of how payments flow in the system around them. Understanding this system is essential to help surgeons recognize the incentives and motivations of other stakeholders in the system.
Elective arthroplasty in a Medicare patient
Hip and knee arthroplasty are common procedures and represent up to 20%-30% of Medicare spending on musculoskeletal conditions. Many of the policies enacted by private insurance companies take their origins in Centers for Medicare & Medicaid Services (CMS) coding and payment policies, so understanding the finances in this case helps understand other clinical scenarios.
In brief: Money flows into the system through patients themselves or other taxpayers in the form of Medicare income tax withholdings (“payroll taxes”), which are paid to CMS. CMS then pays the healthcare facility (“Part A” payment for an inpatient procedure or “Part B” payment for an outpatient procedure) and the provider’s practice group (“Part B” payment).
Payments by a patient into CMS and to the facility
When the surgery is done at the outpatient surgery department of a hospital, the patient’s out-of-pocket cost is capped at $1,632, whereas if the surgery is done at an ambulatory surgery center (ASC), the gap can be as high as $2,102, meaning the patient contribution is higher at an ASC, even if the total amount paid into the system is lower. AAOS supports the Medicare Beneficiary Co-Pay Fairness Act of 2025 (H.R. 3006/S.1776) to extend the hospital outpatient department (HOPD) out-of-pocket cost cap to ASCs as well.
Payment from insurer (CMS) to facility (Medicare Part A)
For patients with Traditional Medicare, prior authorization for surgery is typically not required, although private insurers and Medicare Advantage plans do typically require some form of prior approval. Several factors affect the ultimate payment made.
Medical complexity is included in the diagnosis-related group (DRG) itself, so several DRGs exist for any single diagnosis based on the presence of major complications (MCs) and major complications and comorbidities (MCC). In this hip replacement example, the average national payment rate for DRG 470 (no MCC) is ~$12,300, while the payment for DRG 469 (with MCC) is ~$20,000, representing a 60% increase in payment.
The physical setting of the surgery also plays a role in reimbursement, and procedures performed at an inpatient hospital facility have a higher Part A reimbursement than the same procedure performed at a hospital outpatient department or ASC under Part B. In the case of hip replacement, Part B payments at an ASC are ~60%-70% of what the payments are at a hospital facility.
CMS payments reflect a difference in overall costs based on geographic considerations, due to labor cost adjustments, wage indexes, etc. Depending on the state, there may be as much as a 30% variability in payments.
If the hospital is a teaching institution with a residency program, there is an indirect graduate medical education (GME) payment for the additional resources required. Additionally, some facilities have adjustments made to Medicare payments if the hospital serves a community with a larger share of Medicaid patients, called a disproportionate share increase.
Payment from insurer (CMS) to provider (Medicare Part B)
Beyond the facility, a separate payment is made to the provider performing the procedure. This payment is based on the current procedural terminology, maintained by the American Medical Association. The Part B payment for clinician services is the same for all facilities, and there are fewer variable factors, making this payment similar for all providers across the country.
Hospital and facility expenses
- Major hospital expense categories are broken down into these categories:
- implant costs: may be up to 30%-40% of total spending;
- clinical staff salaries: these costs have gone up 20%-40% in the last four years.
- administrative staff salaries: around 10% of total spending;
- supply costs: around 5%-10% of total spending; and
- physical plant and major equipment: account for 5%-10% of total expenses.
After all these expenses are accounted for, the remaining balance goes toward facility profit. Historically, profit margins for large hospital systems are reported in the 2%-6% range, with margins as high as 6%-10% reported for successful for-profit facilities. Since the pandemic, margins fell substantially, with the median hospital margin in 2022 reported at 0.2%. Margins appear to be recovering, with recent reports in the range of 4% profit. In the hip replacement example, a 4% margin on $12,300 would represent a profit of $492.
Implant costs
Implant costs vary widely, as each hospital system negotiates its own contract with vendors. Hospitals and ASCs often have preferred vendor contracts in which they receive a discount on implants in exchange for commitments related to percentage use and the total number of vendors involved. For a total hip arthroplasty, the mean implant cost for a coated stem with ceramic on poly head and liner costs $4,510. The difference between choosing the lowest and higher cost components could result in price differences up to $1,000, or 20% of the total implant cost.
Private practice expenses
Private practice expenses typically fall into the following ranges:
- staff salaries: 25%-35% of gross income;
- medical supplies/equipment: 10%-20%;
- office space/real estate: 5%-15%;
- billing/coding services: 5%-10%;
- malpractice/insurance: 5%-10%; and
- marketing: 2%-5%.
Anecdotal reports for total overhead rates of 40%-60% are often given, but rates vary widely.
Other costs
In addition to anesthesia services, a significant portion of musculoskeletal spending occurs after discharge from the hospital or ASC.
Post-acute care:
- skilled nursing facility: ~$550/day (up to 20 days fully covered by Medicare Part A, then partial coverage up to day 100);
- inpatient rehabilitation: higher daily costs, but more intensive therapy (Part A);
- outpatient physical therapy: ~$100-$150 per session (covered under Part B, subject to deductible and coinsurance); and
- home health: variable, covered under Part A or B, depending on the service.
- Imaging, medication, and durable medical equipment (DME) costs:
- imaging is covered under Part B;
- medications: Part D covers prescriptions, but many patients face formulary and copay variation;
- DME is covered under Part B with 20% coinsurance after deductible.
Conclusion
Each step in the process is governed by rules that aim to balance access, quality, and cost, but the resulting structure creates a web of incentives that shape the behavior of every stakeholder: hospitals, surgeons, insurers, vendors, and patients.
For surgeons, being literate in the real dollars involved offers a clearer view of how institutional priorities are set and why certain decisions are made. Knowing where the money goes doesn’t just help you understand the system — it empowers you to influence it.
Eric Swart MD, FAAOS, is an orthopaedic trauma surgeon and associate professor at the University of Massachusetts Chan Medical School, where he serves as vice chair of surgical quality at Lahey Hospital & Medical Center. He is a former member of the AAOS Health Care Systems Committee.
Elizabeth Duckworth MD, MBA, is an orthopaedic trauma fellow at Keck School of Medicine of the University of Southern California/Los Angeles General Medical Center. She is a former member of the AAOS Health Care Systems Committee.
Abner Ward, MD, FAAOS, is a board-certified orthopaedic surgeon with sub-specialty fellowship training in hand and upper extremity surgery, orthopaedic sports medicine, and shoulder and elbow surgery. Dr. Ward is an associate professor at the Uniformed Services University of the Health Sciences, an officer in the US Air Force Reserves, and team physician for UC Merced, Merced College, and the Kona Ironman World Championship.
References
- Muoio D. Hospitals’ per-patient labor spend increased 37% from 2019 to Q1 2022. Fierce Healthcare. Published May 12, 2022. Accessed June 3, 2026. https://www.fiercehealthcare.com/providers/hospitals-patient-labor-spend-increased-37-2019-q1-2022
- Southwick R. Hospitals can expect weak margins for the rest of 2023 and into 2024. Chief Healthcare Executive. Published July 2023. Accessed June 3, 2026. https://www.chiefhealthcareexecutive.com/view/hospitals-can-expect-weak-margins-for-the-rest-of-2023-and-into-2024
- Madden B. 2024: the year of health system margin recovery Ð analyzing Q1 2024 hospital performance. Hospitalogy. Published June 3, 2024. Accessed June 3, 2026. https://hospitalogy.com/articles/2024-06-03/health-system-q1-2024-financial-performance-analysis-operating-margin/
- Zuckerman JD, Koli EN, Inneh I, Iorio R. Can a hip and knee adult reconstruction orthopaedic surgeon sustain a practice comprised entirely of Medicare patients? J Arthroplasty. 2014;29(9 Suppl):132-134. doi:10.1016/j.arth.2014.02.041
- Grogan TJ, McCaslin M. Calculating overhead: what it really costs to see a patient. AAOS Now. 2015;9(9).
- Typical net collections for private practice ortho. White Coat Investor Forum. Published July 2023. Accessed June 3, 2026. https://forum.whitecoatinvestor.com/practice-management/404027-typical-net-collections-for-private-practice-ortho
- Private practice overhead. Student Doctor Network Forums. Published October 2021. Accessed June 3, 2026. https://forums.studentdoctor.net/threads/private-practice-overhead.1451686/
- Catanese SJ. Understanding the complexities of overhead in a physician practice. Western Pennsylvania Healthcare News. Published August 7, 2013. Updated August 28, 2023. Accessed June 3, 2026.