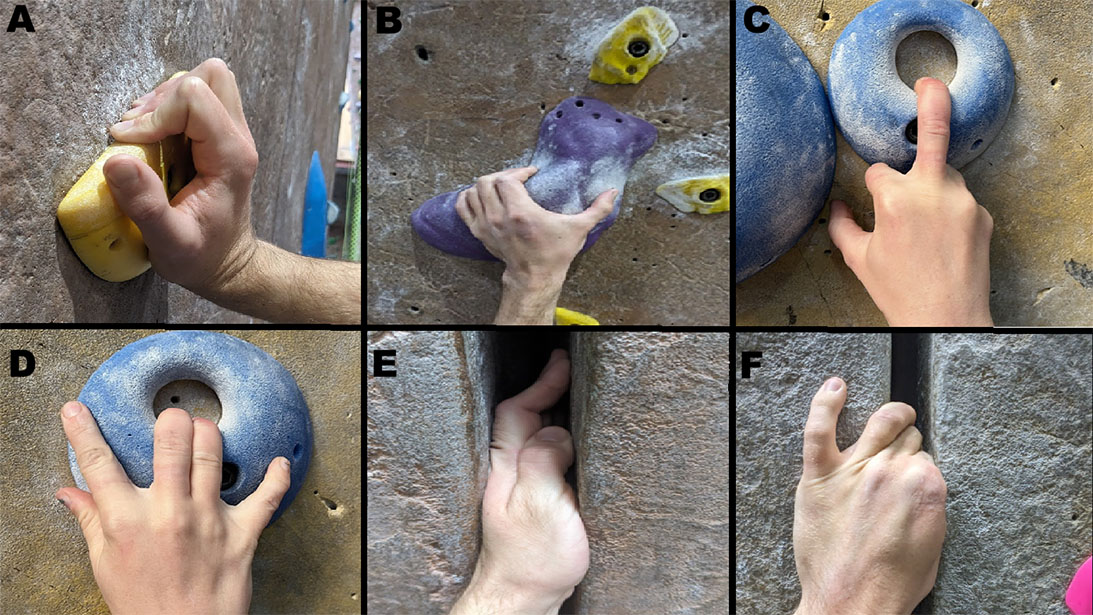
Figure 1. Different types of climbing grips: (A) crimp, (B) sloper pinch, (C) single finger pocket, (D) double finger pocket, (E) hand jam, (F) finger jam
Courtesy of the San Diego Climbing Community
Published 3/28/2026
|
Dori Neill Cage, MD, FAAOS; Abigail Bosco, MPH
Rock climbing is a popular sport around the word and is gaining in popularity. With the rise in indoor climbing facilities, the number and demographics of climbers have expanded. Estimates from 2021 indicate there are more than 10.3 million active climbers in the United States, and as participation rates increase, so does the incidence of climbing-related injuries. The estimated rate of injury is 4.2 injuries per 1,000 hours of climbing. Approximately two-thirds of climbing injuries involve the upper extremities, particularly the hands and fingers. This article reviews hand injuries in climbers, focusing on injury patterns, mechanisms of injury, and treatment guidelines.
Understanding the etiology of injuries is key to their prevention and effective treatment. Climbing injuries occur via several mechanisms within the following categories: overuse or microtrauma, acute trauma, acute supraphysiological loading, and equipment failure or misuse. Overuse or chronic microtrauma is the most common mechanism of injury. Microtrauma may occur as a result of repetitive high loads on tendons, ligaments, and joints of the hands and upper extremities. Trauma due to overuse is estimated to account for approximately 93% of all rock-climbing injuries.
Figure 1. Different types of climbing grips: (A) crimp, (B) sloper pinch, (C) single finger pocket, (D) double finger pocket, (E) hand jam, (F) finger jam
Courtesy of the San Diego Climbing Community
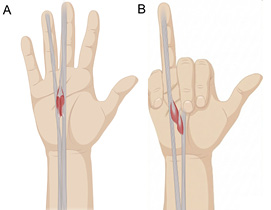
Figure 2. Lumbrical Tear anatomy: (A) intact lumbrical muscle (B) lumbrical muscle tear
Courtesy of the San Diego Climbing Community
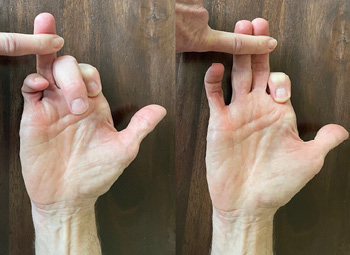
Figure 3. Lumbrical stress
Courtesy of the San Diego Climbing Community
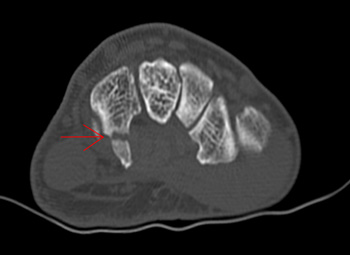
Figure 4. Hook of hamate fracture visualized through CT scan
Courtesy of the San Diego Climbing Community
Technique-specific mechanisms, such as the use of crimp grips and pocket grips, also play a substantial role (Figure 1). Bouldering and sport climbing predispose climbers to hand injuries due to their high force and dynamic movement demands. In contrast, traditional climbing often results in ligament sprains or fractures.
Hand injuries in climbers include flexor pulley injuries, lumbrical strains, carpal tunnel syndrome, hook of hamate fractures, physeal stress injuries, and finger arthritis.
Annular pulley injury, a hallmark injury in climbers, typically occurs when the flexor tendon force is extreme, particularly during a crimp grip, where forces greater than 400 N are exerted on the annular pulley. In a crimp grip, proximal interphalangeal (PIP) joints are flexed more than 90 degrees, and the distal interphalangeal (DIP) joints are hyperextended. Climbers often report a sudden “pop” in the finger followed by pain and swelling. Diagnosis is clinical but can also be identified or confirmed by MRI or ultrasound. An isolated pulley injury can typically be managed nonoperatively with rest, taping, or splinting. Multiple pulley injuries with persistent finger weakness or stiffness may require surgical reconstruction. Tenosynovitis of the long and ring fingers is common among climbers and may mimic pulley injuries, complicating diagnosis. Ultrasound imaging helps differentiate pulley injuries from tenosynovitis.
Another common type of injury is lumbrical injury (Figure 2), which most commonly results from single-finger crimp gripping, particularly involving the long or ring finger. Diagnosis is supported by a positive lumbrical stress test (Figure 3), in which pain is felt during the extension of the affected finger while the adjacent fingers are held in flexion; of note, the pain is not felt when two fingers are extended simultaneously. Management is typically nonoperative, with recovery often taking approximately five to six months.
Other common overuse injuries among climbers are carpal tunnel syndrome (CTS) and pronator syndrome, both of which have a higher incidence in professional climbers and crack climbers (those who specialize in climbing rock cracks by jamming hands and arms into the fissures). Repetitive wrist flexion, digital tendon swelling, and forearm muscle hypertrophy contribute to median nerve compression in the forearm and wrist. Management involves splinting, ergonomic grip modification, steroid injections, and surgical decompression. If an individual requires surgical decompression, they can often return to rock climbing within six to eight weeks post carpal tunnel release.
Falls, slips, and dynamic moves can lead to a variety of acute traumatic injuries
Acute traumatic injuries can occur from falls (e.g., falling on an outstretched hand), sudden slips while gripping holds, or violent dynamic moves. Falls or impacts can lead to fractures or dislocations. For example, a sudden slip from a Sloper grip (Figure 1B) can result in hamate hook fracture, thumb medial collateral ligament (MCL) injury, or finger pulley injury. Unlike injury in contact sports, in which a hamate fracture may be due to a direct blow, hook of hamate fractures are reported among climbers using undercling holds or other forceful grip techniques. Injury presents as ulnar-sided palm pain and can be missed on standard radiographs (Figure 4). Nondisplaced fractures heal with immobilization, but persistent symptoms or displacement often warrant surgical treatment of the fracture. Surgical excision may result in finger flexion weakness and should be avoided in this population when possible. Triangular fibrocartilage complex (TFCC) tears are an additional cause of ulnar-sided pain; they are seen with an increased incidence in climbers and may be confirmed through MRI imaging. Another common type of acute trauma injury occurs as a collateral ligament injury to the thumb metacarpophalangeal (MP) joint or long finger PIP joint. Surgical indications for long finger PIP collateral ligament injuries are not well defined.
Growth-related vulnerabilities contribute to distinctive injuries in pediatric climbers
Pediatric climbers are at risk for unique injuries. Of particular concern are Salter-Harris 3 fractures of the middle phalanges. A higher incidence is seen in children who participate in bouldering and intensive finger strengthening. These fractures may present as pain, swelling, decreased range of motion, or angular deformity rather than an acute event. MRI is recommended for individuals who present with any of these symptoms but have normal radiographs. Early identification is critical to prevent growth arrest. Management is primarily nonoperative, including rest and splinting.
Years of climbing can contribute to progressive structural changes in the DIP and PIP joints
Long-term climbers often exhibit radiographic changes such as cortical thickening and osteophyte formation in the DIP joints and the PIP joints. While these developments do not always correlate with symptoms, some veteran climbers report stiffness or intermittent pain in the absence of acute injury. Conservative care with NSAIDs, grip modification, and steroid injections during flare-ups are typically effective. Severe joint deformity may rarely require surgical intervention.
Conclusion
Assessment of climbing injuries should specifically address the climber’s history of injury, grip type, climbing style, and training regimen. In addition to a thorough physical examination, diagnostic imaging such as radiograph, CT, MRI, or ultrasound can facilitate proper and accurate diagnosis of climbing injuries. Preventive measures, such as proper warm-ups or use of open hand grips, may greatly reduce the frequency of injury. When injury occurs, treatment should address the specific diagnosis. Rehabilitation should emphasize hand therapy, muscle strengthening, and progressive load return.
As rock climbing continues to grow in popularity, hand and upper extremity injuries will become increasingly relevant to orthopaedic practice. A comprehensive understanding of climbing biomechanics and injury patterns will allow clinicians to effectively treat these injuries.
Dori Neill Cage, MD, FAAOS, president of San Diego Hand Specialists, is a private practice orthopedic hand and upper extremity surgeon
Abigail Bosco, MPH, is a research assistant at SDSU Research Foundation. She will begin her medical education at UCLA in the fall.
Special thanks to author Laura Sims, MD, as the primary reference and to the San Diego climbing community for the photography.
References
- Backe S, Ericson L, Janson S, Timpka T. Rock climbing injury rates and associated risk factors in a general climbing population. Scand J Med Sci Sports. 2009;19(6):850856.
- Chen K, Sundaram S, Lo DF, Gawash A, Papachristou C, Raja AE. Scaling new heights: A prospective survey of rock climbing’s impact on mental health. Discov Ment Health. 2025;5(1):29. doi:10.1007/s44192-025-00154-0
- Fufa D. Recovery milestones for carpal tunnel release surgery. SportsHealth. Published August 1, 2017. Accessed March 10, 2026. https://www.sports-health.com/treatment/hand-and-wrist-injury-treatment/recovery-milestones-carpal-tunnel-release-surgery
- Kubiak EN, Klugman JA, Bosco JA. Hand injuries in rock climbers. Bull NYU Hosp Jt Dis. 2006;64(3-4):172177.
- Lutter C, Schweizer A, Hochholzer T, Bayer T, Schöffl V. Pulling harder than the hamate tolerates: Evaluation of hamate injuries in rock climbing and bouldering. Wilderness Environ Med. 2016;27(4):492499. doi:10.1016/j.wem.2016.09.003
- Pastor T, Schweizer A, Andronic O, et al. A life dedicated to climbing and its sequelae in the fingers—a review of the literature. Int J Environ Res Public Health. 2022;19(24):17050.
- Peters P. Nerve compression syndromes in sport climbers. Int J Sports Med. 2001;22(8):611617.
- Pidgeon T. Hook of the hamate fracture of the wrist. OrthoInfo—AAOS. Published March 2024. Accessed March 10, 2026. https://www.orthoinfo.org/en/diseases--conditions/hook-of-the-hamate-fracture-of-the-wrist/
- Schöffl VR. Tendon injuries in the hands in rock climbers: Epidemiology, anatomy, biomechanics and treatment—an update. Muscles Ligaments Tendons J. 2020;10(2):233243.
- Schöffl VR, Lutter C, Lang HC, Perl M, Moser O, Simon M. Efficacy of a new treatment algorithm for capsulitis of the fingers in rock climbers. Front Sports Act Living. 2025;7:1497110. doi:10.3389/fspor.2025.1497110
- Schweizer A. Sport climbing from a medical point of view. Swiss Med Wkly. 2012;142:w13688.
- Sims LA. Upper extremity injuries in rock climbers: Diagnosis and management. J Hand Surg Am. 2022;47(7):662672. doi:10.1016/j.jhsa.2022.01.009