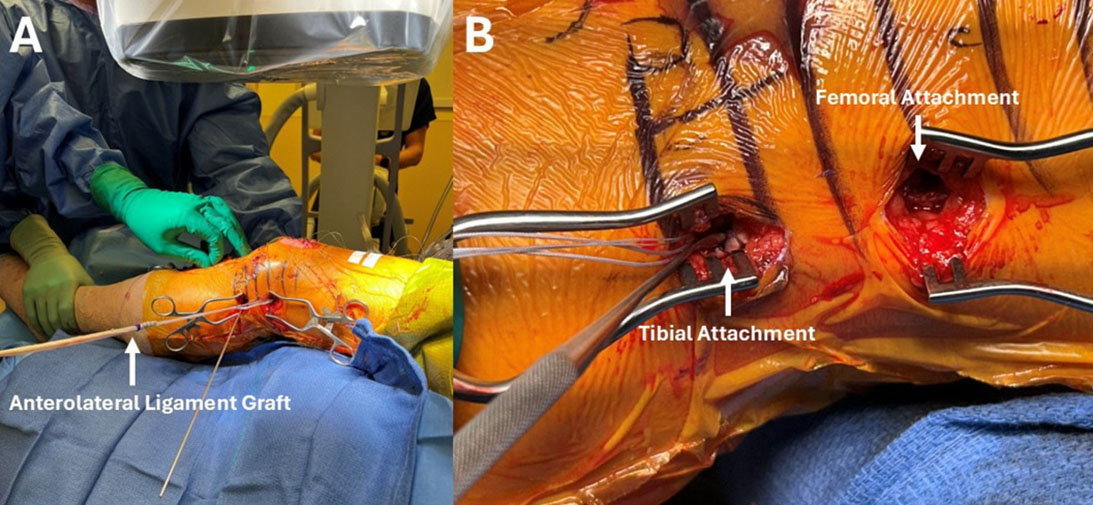
Figure 1. An anterolateral ligament reconstruction with ACL reconstruction. A tendon allograft is delivered and docked at the lateral femoral attachment (A). The final anterolateral ligament reconstruction with its completed femoral attachment and a singular tibial attachment between Gerdy’s tubercle and fibular head (B).
Courtesy of Richard Ma, MD, FAAOS
Published 3/29/2026
|
William Ma, BS; Richard Ma, MD
While the outcome of anterior cruciate ligament (ACL) reconstruction is generally successful, clinical failure, including secondary injury of the ACL graft or excessive laxity of the repaired knee, still occurs with frequency. Patient-specific and technical factors may contribute to this overall risk of failure. Certain patient populations are at high risk for clinical failure after ACL surgery. Specifically, younger individuals, female sex, and high activity level (e.g., sports participation) have all been associated with an increased risk of ACL graft reinjury or need for revision surgery after ACL reconstruction. In their systematic review and meta-analyses of 19 studies, Wiggins et al. found that individuals younger than 25 who returned to sports were associated with a 23% rate of secondary ACL injury. Individuals with high-grade preoperative knee laxity (i.e., >10 mm anterior drawer and Lachman or 3+ pivot) have also been associated with a significantly greater risk for revision ACL surgery.
In addition to patient risk factors, there are also technical aspects in the evolution of ACL surgery that may pose an increased demand, and therefore risk, for the ACL graft. There has been a paradigm shift in contemporary ACL reconstruction toward anatomic ACL footprint restoration with the goal of recreating the native ACL footprint to better approximate normal knee kinematics and stability with ACL reconstruction. The results of this approach are higher forces on the ACL graft and graft anisometry. Some clinical studies have hypothesized that the increased demand on the ACL graft with anatomic ACL reconstruction may impact the relative risk of graft failure after anatomic ACL reconstruction, although this is a topic of ongoing debate. The combination of a continued higher rate of secondary ACL injuries or graft failure within certain patient populations, despite modern ACL reconstruction techniques, are among the reasons clinicians continue to pursue improvements with ACL surgery.
Anatomy and biomechanics of lateral extra-articular structures in ACL injury and surgery
The anterolateral ligament complex includes the anterolateral ligament (ALL), iliotibial band (ITB), Kaplan fibers, and the anterolateral capsule. Claes et al. demonstrated the ALL is a distinct lateral extracapsular ligamentous structure and hypothesized that ALL served as a secondary stabilizer to the ACL in resisting anterior translation and internal tibial rotation and minimized the pivot shift phenomenon. The ALL has its femoral origin either near the origin of the lateral collateral ligament (LCL) or proximal posterior to the LCL. Its tibial attachment is approximately midway between Gerdy's tubercle and the fibular styloid (24.7 mm posterior to the center of Gerdy's tubercle and 26.1 mm proximal to the anterior margin of the fibular head). In biomechanical studies, it was noted that sectioning the anteromedial and posterolateral bundles of ACL often only produced grade I or II pivots, while sectioning the ALL alone produced a grade I pivot. A high-grade pivot (e.g., grade III) was only produced when both the ALL and ACL were sectioned. These works highlighted the potential crucial role of the ALL working alongside the ACL in stabilizing the knee against pivot shift rotatory forces.
Two LEAPs provide similar stability with ACLR
Two widely used iterations of lateral extra- articular procedures (LEAPs) include lateral extra-articular tenodesis (LET) and the anterolateral ligament reconstruction (ALLR) with a tendon graft. The most common type of LET is the modified Lemaire procedure in which a 1 cm wide by 8 cm long strip of the IT band is left attached distally to Gerdy's tubercle, released proximally, and passed deep to the LCL. The ITB graft is then fixed to the femur posteriorly and proximal to the LCL using a staple, screw, or anchor. In contrast, ALLR can involve passing a tendon graft superficially or deep to the LCL (Figure 1). The graft is then secured to the femur proximally and subsequently to the tibia either as a singular point between Gerdy's tubercle and the fibular head or a two-point attachment at the proximal tibia. Cadaveric and clinical studies comparing LET and ALLR have demonstrated near equivalence in terms of biomechanical performance and clinical outcomes. Both techniques appear effective in restoring knee kinematic in conjunction with ACL reconstruction. In a recent network meta-analysis of available randomized controlled trials (RCT), both LET and ALLR were effective in reducing pivot shift and improving patient-reported outcome measures relative to isolated ACL reconstruction alone.
Clinical indications for adding LEAPs for ACL reconstruction
Current indications for the addition of LEAPs with ACL surgery are expanding as the clinical evidence evolves. Clinical indications include individuals with high-grade ACL or physiologic knee laxity (i.e., 3+ Lachman and/or pivot shift, knee hyperextension ≥10 degrees, physiologically lax females) and patients undergoing revision ACL reconstruction. LEAPs may also be considered in ACL reconstruction with at-risk grafts (e.g., hamstring autograft). A systematic review of 23 studies identified that the most common indications for LEAPs are either a positive pivot shift grade (≥ 2), patients requiring revision ALCR, ligamentous laxity (Breighton score > 4), participation in sports, and patients younger than 25.
Comparative studies on outcomes of LEAPs with ACL reconstruction
The current clinical literature suggests there is a significant risk reduction of reinjury with the addition of LEAPs to ACL reconstruction. A multicenter RCT of 618 patients showed that the addition of LET to ACL reconstruction with hamstring tendon (HT) autograft reduced the reinjury rate to 4% compared to 11% with ACL reconstruction alone. Another RCT evaluated 556 patients who were randomized to either isolated ACLR with bone-patellar tendon-bone autografts or ACL reconstruction (HT autograft) with ALLR. The authors reported the lower graft reinjury rate with HT and ALLR group (4.2%) versus ACL reconstruction alone (10.3%) at five years from surgery. Across the literature, when ACLR was combined with either LET or ALLR, patients were found to have better rotational stability, decreased likelihood of graft failure, and improved return to play.
LEAP limitations or risks
The potential downsides of LEAPs include the cost of the extra operative time and the implant used. However, recent studies that have modeled the addition of LET to ACLR have suggested economic benefit due to the reduced risk of revision. The impact of adding a lateral restraint on the long-term health of the knee is not fully known. However, recent systematic review and meta-analysis studies have shown that the addition of LET was not associated with increased risk of knee osteoarthritis (OA) versus ACLR alone. LET may also have a protective effect in terms of OA risk in post-meniscectomized knees.
Conclusion
While the outcomes of ACL reconstruction surgery are good, certain patient populations are at an increased risk for failure after primary ACL reconstruction. The ALL is an important structure that can work alongside the ACL to control rotatory knee stability in the setting of ACL injuries. Both LETs and ALLR have been shown to be effective in reducing clinical failure after ACL reconstruction, and the indications for adding LEAPs to ACL surgery are likely to expand given its positive impacts on surgery outcomes.
William Ma, BS, is a medical student at the University of Missouri School of Medicine.
Richard Ma, MD, FAAOS, is the Gregory L. and Ann L. Hummel Distinguished Professor and Director of Sports Medicine in the Department of Orthopaedic Surgery at the University of Missouri. He also serves as a member of the AAOS Now Editorial Board.
References
- Wiggins AJ, Grandhi RK, Schneider DK, Stanfield D, Webster KE, Myer GD, et al. Risk of secondary injury in younger athletes after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med. 2016;44(7):1861‑1876. doi:10.1177/0363546515621554
- Magnussen RA, Reinke EK, McMahon KE, Spindler KP, et al. Effect of high‑grade preoperative knee laxity on anterior cruciate ligament reconstruction outcomes. Am J Sports Med. 2016;44(12):3077‑3082. doi:10.1177/0363546516656835
- Zhao D, Pan JK, Lin FZ, Luo MH, Liang GH, Zeng LF, et al. Risk factors for revision or rerupture after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med. 2023;51(11):3053‑3075. doi:10.1177/03635465221119787
- Lubowitz, JH, Anatomic ACL reconstruction produces greater graft length change during knee range-of-motion than transtibial technique. Knee Surg Sports Traumatol Arthrosc. 2014;22(5):1190-1195.
- Araujo PH, Asai S, Pinto M, Protta T, Middleton K, Linde‑Rosen M, et al. ACL graft position affects in situ graft force following ACL reconstruction. J Bone Joint Surg Am. 2015;97(21):1767‑1773. doi:10.2106/JBJS.N.00539
- Rahr‑Wagner L, Thillemann TM, Pedersen AB, Lind M, et al. Increased risk of revision after anteromedial compared with transtibial drilling of the femoral tunnel during primary anterior cruciate ligament reconstruction: results from the Danish Knee Ligament Reconstruction Register. Arthroscopy. 2013;29(1):98‑105. doi:10.1016/j.arthro.2012.09.009
- Gabr A, Khan M, Kini SG, Haddad F, et al. Anteromedial portal versus transtibial drilling techniques for femoral tunnel placement in arthroscopic anterior cruciate ligament reconstruction: radiographic evaluation and functional outcomes at 2 years follow-up. J Knee Surg. 2023;36(13):1309‑1315. doi:10.1055/s‑0042‑1755358
- Desai N, Andernord D, Sundemo D, Alentorn‑Geli E, Musahl V, Fu FH, et al. Revision surgery in anterior cruciate ligament reconstruction: a cohort study of 17,682 patients from the Swedish National Knee Ligament Register. Knee Surg Sports Traumatol Arthrosc. 2017;25(5):1542‑1554.
- Kraeutler MJ, Welton KL, Chahla J, LaPrade RF, Krych AJ, Arendt EA, et al. Current concepts of the anterolateral ligament of the knee: anatomy, biomechanics, and reconstruction. Am J Sports Med. 2018;46(5):1235‑1242. doi:10.1177/0363546517701920
- Claes S, Vereecke E, Maes M, Victor J, Verdonk P, Bellemans J. Anatomy of the anterolateral ligament of the knee. J Anat. 2013;223(4):321‑328. doi:10.1111/joa.12087
- Claes S. The anterolateral ligament (ALL): anatomy, biomechanics, and function. Presented at: ArthroParis 2014; 2014; Paris, France.
- Getgood AMJ, Bryant DM, Litchfield R, Heard M, McCormack RG, Rezansoff A, et al. Lateral extra‑articular tenodesis reduces failure of hamstring tendon autograft anterior cruciate ligament reconstruction: 2‑year outcomes from the STABILITY study randomized clinical trial. Am J Sports Med. 2020;48(2):285‑297. doi:10.1177/0363546519896333
- Smith PA, Thomas DM, Pomajzl RJ, Bley JA, Pfeiffer FM, Cook JL. A biomechanical study of the role of the anterolateral ligament and the deep iliotibial band for control of a simulated pivot shift with comparison of minimally invasive extra‑articular anterolateral tendon graft reconstruction versus modified Lemaire reconstruction after anterior cruciate ligament reconstruction. Arthroscopy. 2019;35(5):1473‑1483. doi:10.1016/j.arthro.2018.11.011
- Park YB, Lee HJ, Cho HC, Pujol N, Kim SH, et al. Combined lateral extra‑articular tenodesis or combined anterolateral ligament reconstruction and anterior cruciate ligament reconstruction improves outcomes compared to isolated reconstruction for anterior cruciate ligament tear: a network meta-analysis of randomized controlled trials. Arthroscopy. 2023;39(3):758‑776. doi: d10.1016/j.arthro.2022.11.032
- Sonnery‑Cottet B, Carrozzo A, Poilvache H, Fayard JM, Freychet B, Thaunat M, et al. Anterior cruciate ligament reconstruction combined with anterolateral ligament reconstruction using hamstring autograft versus anterior cruciate ligament reconstruction using bone‑patellar tendon‑bone autograft: a randomised controlled trial with 5‑year follow‑up. Lancet Reg Health Eur. 2025;62:101561. doi:10.1016/j.lanepe.2025.101561
- Varady NH, Oeding JF, Inclan PM, Ranawat AS, Strickland SS, Pearle AD, Rodeo SA, Williams III, RJ. Adding a lateral extra-articular tenodesis is cost-effective in primary anterior cruciate ligament reconstruction: a Markov analysis. Arthroscopy. 2025; 41(11):4772-4785.
- Gkekas NK, Stamiris D, Koutalos AA, Chantes I, Komnos GA, Hantes M. Combining ACL reconstruction with lateral extra-articular tenodesis reduces long-term osteoarthritis risk versus isolated ACL reconstruction: a systematic review and meta-analysis. J Bone Joint Surg Am. 2026 Feb 4;108(3):193-201. doi: 10.2106/JBJS.25.00907.
- Bouchard MD, Haque O, Cruickshank M, Vivekanantha P, Tapasvi S, Meena A, de Sa D. Ten-year outcomes of combined ACLR and lateral extra-articular tenodesis: A systematic review. Knee Surg Sports Traumatol Arthrosc. 2025 Dec 26. doi: 10.1002/ksa.70231