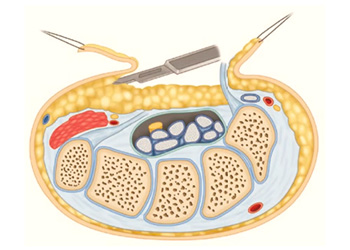
Figure 1: A diagram of the hypothenar fat pad flap
Published 3/28/2026
|
Leslie Schwindel, MD, FAAOS
Editor's note: The following article is a review of a video available via the AAOS Orthopaedic Video Theater (OVT). AAOS Now will routinely review “OVT Plus” videos, which are vetted by topic experts and offer CME. For more information, visit aaos.org/OVT.
Carpal tunnel syndrome is one of the most prevalent focal mononeuropathies, constituting 90% of neuropathy cases. The incidence in the general population is reported to range from 1%-5% and is one of the most common conditions treated by orthopaedic surgeons. Three percent to 19% of patients experience recurrence of carpal tunnel syndrome after primary carpal tunnel release surgery.
Figure 1: A diagram of the hypothenar fat pad flap

Figure 2: The fat pad flap was mobilized to ensure adequate coverage of the median nerve and secured to the undersurface of the radial TCL leaflet remnant with 4‑0 Vicryl horizontal mattress sutures.
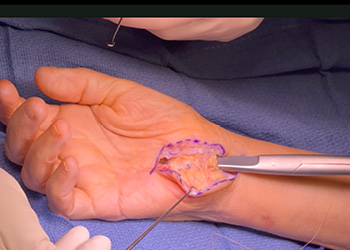
Figure 3: A tourniquet was tensioned so that undue pressure was not placed on the nerve, and it glided freely underneath the fat pad flap.
Recurrence is defined as a return of numbness after a symptom-free interval following carpal tunnel release. Common causes of recurrence include alternative pathologies such as a tumor, systemic disease (i.e., diabetes mellitus), or distal radius fracture. Additionally, factors related to the index surgery can lead to recurrence, including an incomplete release of the transverse carpal ligament, recurrent tenosynovitis, perineural scarring, and/or reconstitution of the transverse carpal ligament.
Treatment options for recurrent carpal tunnel syndrome are largely surgical. Nonsurgical intervention is not typically recommended to prevent further symptomatic progression and more permanent neurologic damage. Revision surgery may include a simple revision decompression through a standard open approach if the recurrence is from pathology unrelated to the index procedure or if the index procedure was performed endoscopically.
However, in patients with an open index procedure and/or recurrence attributed to factors from the index surgery, the nerve will likely be significantly scarred, so it is beneficial to provide some type of coverage to create a barrier to scar tissue reforming. There are many acceptable forms of coverage, the most prevalent in the literature being synovial flap, muscle flap, vascularized fascia, synthetic flap, and hypothenar fat pad flap, among others.
In the AAOS OVT video “The Hypothenar Fat Pad Flap for Recurrent Carpal Tunnel Syndrome,” the authors demonstrate the surgical technique for a hypothenar fat pad flap. In short, this flap mobilizes a pad of vascularized fat from the hypothenar eminence and interposes it between the median nerve and the remnant radial leaflet of the transverse carpal ligament. This prevents scar tissue formation, encourages neovascularization, and allows for smooth gliding of the nerve.
In the video, the authors use a personal example of a patient who underwent a carpal tunnel release and experienced a recurrence in symptoms. The previous surgical incision was used for exposure but was extended slightly proximally and distally. Dissection was carried through the antebrachial fascia and the median nerve identified in relatively fresh territory. They confirmed the transverse carpal ligament (TCL) had reconstituted. It was incised ulnarly off the hook of the hamate so that they were cutting directly over the flexor tendons rather than over the nerve.
Flexor synovium was released, and neurolysis completed, releasing the nerve from the radial leaflet of the transverse carpal ligament. The nerve was freed from proximal to distal, taking care to avoid the recurrent motor branch and palmar digital branches. Dissection was carried distally until the superficial arch with its overlying fat was identified. To complete the hypothenar fat pad, a 10 blade was used to elevate the hypothenar fat pad, elevating the hypothenar skin flap, leaving 1-2 mm of fat on the skin to preserve the vascularity of the subdermal plexus (Figure 1).
The fat pad flap was mobilized, ensuring it would move well and cover the median nerve. A 4-0 Vicryl suture was used to secure the fat pad flap to the undersurface of the radial leaflet remnant of the TCL using horizontal mattress stitches (Figure 2). Once the fat pad was secured and the nerve covered, a tourniquet was dropped to confirm good vascularity of the flap. This tourniquet was tensioned so that undue pressure was not placed on the nerve, and it glided freely underneath the fat pad flap (Figure 3). Standard skin closure was performed, and a short arm splint was applied for two weeks, after which the patient began occupational therapy.
The authors describe personal success with this technique but also remark on several studies confirming good outcomes reported in the literature. They specifically mention a meta-analysis published in the Journal of Hand Surgery in 2022, analyzing 14 studies. Treatment groups included simple decompression with or without neurolysis, autologous fat transfer, hypothenar fat pad, pedicled or free flap, and “other.” When comparing preoperative and postoperative patient-reported outcome measures — Boston Carpal Tunnel Questionnaire (BCTQ) and Visual Analog Scale (VAS) — there was a clinically significant improvement in the BCTQ symptom severity scores for the hypothenar fat pad group and the autologous fat transfer groups compared to other treatment groups. In summary, the hypothenar fat pad flap is a reliable way to obtain local coverage of the median nerve in patients with recurrent carpal tunnel syndrome. It uses the patient’s own tissue, avoids the need for synthetic grafts, contains costs, and is relatively simple to perform, with very good, published outcomes. Any surgeon who performs carpal tunnel releases would benefit from mastering this technique.
Leslie Schwindel, MD, FAAOS, is a board-certified orthopaedic surgeon specializing in joint replacement, athletic injuries, pediatric injuries, fracture care, muscle/tendon injuries, and bone and joint health. She practices at Lake Cumberland Orthopedics and Surgical Podiatry in Somerset, Kentucky. She is also a member of the AAOS Now Editorial Board.
Sevy JO, Reddog EE, Sina R, Varacallo MA. Carpal Tunnel Syndrome. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. Updated October 29, 2023. Available from: https://www.ncbi.nlm.nih.gov/books/