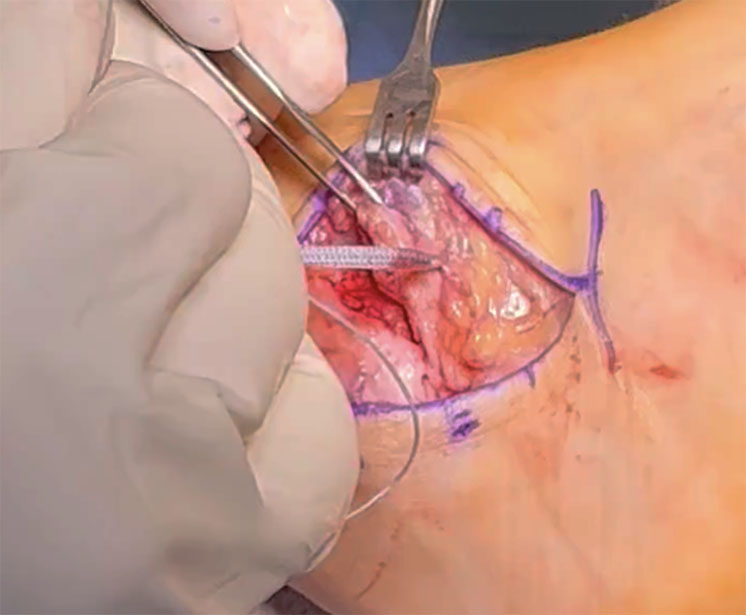
Figure 1: Passing the suture tape through the anterior talofibular ligament (ATFL) and retinaculum. The suture tape is anchored into the talus and pulled out through the cuff of ATFL tissue. It will be secured to the distal fibula after the reconstruction of the ATFL is completed.
Courtesy of Eric W. Tan, MD
Published 3/30/2026
|
Madeleine Orringer, MD; Eric W. Tan, MD
Chronic lateral ankle instability represents a significant burden for athletes. An estimated 20%-40% of individuals who experience an acute lateral ankle sprain will develop chronic ankle instability, characterized by recurrent sprains and persistent pain that can limit athletic performance.
For competitive athletes, prolonged recovery times can profoundly impact their season and career trajectory. Consequently, return-to-play timing has become a critical postoperative outcome measure. Suture tape augmentation of the modified Brostrom procedure has emerged as a promising adjunct that may facilitate accelerated rehabilitation and earlier return to competition.
Figure 1: Passing the suture tape through the anterior talofibular ligament (ATFL) and retinaculum. The suture tape is anchored into the talus and pulled out through the cuff of ATFL tissue. It will be secured to the distal fibula after the reconstruction of the ATFL is completed.
Courtesy of Eric W. Tan, MD
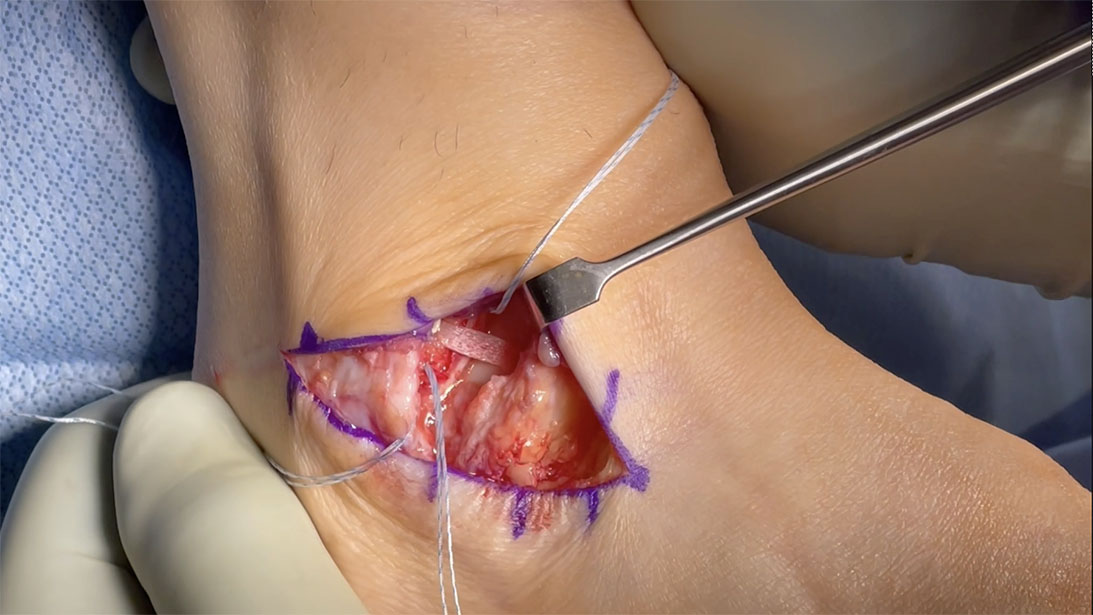
Figure 2: New material has been developed, including a synthetic, degradable matrix woven from wet-spun fibers of polycaprolactone base-polyurethane urea (PUUR, Flexband®, Artelon, Marietta, GA). Similar to Suture tape augmentation, the Flexband is placed across from the talus to the fibula. The suture anchors of the fibula will be used to reconstruct the anterior talofibular ligament tissue cuff.
Courtesy of Taggart Gauvain, MD, FAAOS
The evolution of suture tape augmentation
Suture tape augmentation was popularized in the 2010s as a method to reinforce traditional Brostrom or modified Brostrom-Gould lateral ankle ligament reconstruction. The technique involves placing a high-strength, nonabsorbable suture tape secured with knotless anchors that parallel the reconstructed anterior talofibular ligament (ATFL) (Figure 1).
The biomechanical findings are compelling: Cadaveric studies have demonstrated that suture tape augmentation provides ultimate load-to-failure strength of 250-315 N, exceeding the native ATFL strength of approximately 154 N. Similarly, construct stiffness with augmentation (21-31 N/mm) matches or exceeds native ligament stiffness (14.5 N/mm). This enhanced mechanical strength theoretically protects the biological repair during the vulnerable early postoperative period, permitting more aggressive rehabilitation protocols and functional loading.
Clinical evidence on return to play
The clinical literature on return to play after suture tape augmentation has expanded recently, although it remains dominated by retrospective cohort studies, case series, and systematic reviews. Prospective randomized controlled trials are scarce, limiting the strength of current evidence. Nevertheless, emerging data suggest a consistent trend toward accelerated recovery.
In a multicenter randomized trial involving 119 patients, Kulwin et al. demonstrated that suture tape augmentation enabled return to preinjury level of activity at 13.3 weeks compared to 17.5 weeks for traditional modified Brostrom (P = 0.001). Similarly, systematic reviews report athletes undergoing augmented repairs often return to sport at eight to 12 weeks when following aggressive rehabilitation protocols, compared to the historical time frame of 12 to 24 (or more) weeks for nonaugmented repairs. These studies define return to play as return to the same or higher level of sport and typically use patient-reported outcome measures (PROMs) to assess readiness, including the Foot and Ankle Ability Measure (FAAM), Tegner Activity Scale, and Ankle Ligament Reconstruction-Return to Sport After Injury scale.
Multiple studies have confirmed that both augmented and nonaugmented techniques produce excellent functional outcomes at intermediate and long-term follow-up. PROMs, including the FAAM and American Orthopaedic Foot and Ankle Society (AOFAS) scores, improve significantly with both techniques. Importantly, when differences exist, they typically favor augmentation primarily in the early postoperative period (three to six months), with outcomes converging beyond 12 to 24 months. This finding suggests the primary benefit of augmentation lies in facilitating earlier functional recovery.
The available randomized controlled trial (RCT) data, while limited, generally support the safety and efficacy of augmentation. Porter et al. conducted a five-year RCT comparing ligament augmentation reconstruction system (LARS) augmentation to modified Brostrom- Gould repair, finding superior Foot and Ankle Outcome Scores and higher Tegner Activity Scale scores in the augmented group, with zero failures compared to two in the traditional repair group. A systematic review of three randomized trials, involving 235 patients, found higher postoperative sports activity scores in suture tape groups, with comparable overall functional outcomes.
Complications and safety profile
Regarding safety, systematic reviews report no major differences in overall complication rates between augmented and nonaugmented repairs. However, the complication profiles differ slightly. Recurrence of instability and revision surgeries tend to occur more frequently after traditional Brostrom repair, while peroneal nerve and tendon irritation appear more often with suture tape constructs. In the largest randomized trial, complication rates were 8.5% for modified Brostrom versus 1.7% for suture tape augmentation, though this difference did not reach statistical significance (P = 0.12). These findings suggest that when performed properly, augmentation does not introduce prohibitive risks.
Practical implications
For orthopaedic surgeons counseling athletes about surgical options, suture tape augmentation offers several potential advantages: The enhanced biomechanical strength permits accelerated rehabilitation protocols, including earlier weight-bearing and functional exercises. Studies using aggressive postoperative protocols after surgical fixation with suture tape augmentation report excellent outcomes, with patients achieving single-leg hop and heel-raise capacity at six weeks postoperatively. This type of outcome is particularly valuable for high-level athletes with time-sensitive competition schedules or professional obligations.
However, decision-making should remain holistic and patient specific. Important factors to consider include competitive level, tissue quality, body mass index, history of prior ankle surgery, and presence of generalized ligamentous laxity. Suture tape augmentation may be especially beneficial in revision cases as well as in patients with relative contraindications to traditional repair, including those with generalized ligamentous laxity, elite athletes requiring rapid return, or patients with poor tissue quality.
Surgeons should also counsel patients about the limitations of current evidence. Despite promising early results, the long-term superiority of augmentation over traditional repair remains uncertain. Furthermore, the existing literature suffers from significant heterogeneity in surgical technique, rehabilitation protocols, and outcome definitions, making direct comparisons challenging.
Need for standardized research and future directions
Moving forward, the field would benefit from standardized return-to-play definitions that distinguish between return to training, return to competition, and return to preinjury performance level. Additionally, large randomized controlled studies and research incorporating sport-specific outcome measures would provide more granular insights into recovery trajectories across different athletic endeavors.
Furthermore, given that the augmented construct is stiffer than the native ligament, data-driven guidance on intraoperative tensioning is important to avoid soft tissue imbalance and range-of- motion restrictions.
Novel biomaterials, including a synthetic, degradable matrix woven from wet-spun fibers of polycaprolactone base-polyurethane urea, are now commercially available and provide a biological scaffold for integration and remodeling while also having an elastic modulus closer to the native ligament (Figure 2). This may better mimic the native tissue mechanics while reducing the potential for stress shielding. While early results are promising, further studies are needed to determine the clinical benefit of these newer materials.
Conclusion
Suture tape augmentation of the modified Brostrom procedure represents a valuable addition to the surgical armamentarium for chronic lateral ankle instability. The technique appears to facilitate accelerated rehabilitation and earlier return to play. For athletes, suture tape augmentation offers a promising option supported by growing evidence. Orthopaedic surgeons should engage in shared decision making that considers individual patient factors. While early results are encouraging, definitive evidence of superiority in return-to-competition rates or long-term outcomes requires completion of large, prospective comparative trials with standardized protocols. Until then, surgeons can counsel patients augmentation represents a safe, effective technique that may expedite recovery without compromising long-term stability or function.
Madeleine Orringer, MD, is an orthopaedic surgery resident at the University of Southern California in Los Angeles, California.
Eric W. Tan, MD, is a foot and ankle orthopaedic surgeon and associate professor of orthopaedic surgery at the University of Southern California in Los Angeles, California.
References
- Martin RL, Davenport TE, Fraser JJ, et al. Ankle stability and movement coordination impairments: lateral ankle ligament sprains revision 2021. J Orthop Sports Phys Ther. 2021;51(4):CPG1‑CPG80. doi:10.2519/jospt.2021.0302.
- Hertel J, Corbett RO. An updated model of chronic ankle instability. J Athl Train. 2019;54(6):572‑588. doi:10.4085/1062-6050-344-18.
- Wikstrom EA, Hubbard‑Turner T, McKeon PO. Understanding and treating lateral ankle sprains and their consequences: a constraints‑based approach. Sports Med. 2013;43(6):385‑393. doi:10.1007/s40279-013-0043-z.
- Wittig U, Hohenberger G, Ornig M, et al. Improved outcome and earlier return to activity after suture tape augmentation versus Broström repair for chronic lateral ankle instability? A systematic review. Arthroscopy. 2022;38(2):597‑608. doi:10.1016/j.arthro.2021.06.028.
- Viens NA, Wijdicks CA, Campbell KJ, LaPrade RF, Clanton TO. Anterior talofibular ligament ruptures, part 1: biomechanical comparison of augmented Broström repair techniques with the intact anterior talofibular ligament. Am J Sports Med. 2014;42(2):405‑411. doi:10.1177/0363546513510141.
- Martin KD, Andres NN, Robinson WH. Suture tape augmented Broström procedure and early accelerated rehabilitation. Foot Ankle Int. 2021;42(2):145‑150. doi:10.1177/1071100720959015.
- Kulwin R, Watson TS, Rigby R, Coetzee JC, Vora A. Traditional modified Broström vs suture tape ligament augmentation. Foot Ankle Int. 2021;42(5):554‑561. Doi:10.1177/1071100720976071.
- Lan R, Piatt ET, Bolia IK, et al. Suture tape augmentation in lateral ankle ligament surgery: current concepts review. Foot Ankle Orthop. 2021;6(4):24730114211045978. doi:10.1177/24730114211045978.
- Li J, Qi W, Yun X, et al. Comparison of modified Broström procedure with or without suture tape augmentation technique for chronic lateral ankle instability. Biomed Res Int. 2022;2022:6172280. doi:10.1155/2022/6172280.
- Ulku TK, Kocaoglu B, Tok O, Irgit K, Nalbantoglu U. Arthroscopic suture‑tape internal bracing is as safe as arthroscopic modified Broström repair in the treatment of chronic ankle instability. Knee Surg Sports Traumatol Arthrosc. 2020;28(1):227‑232. doi:10.1007/s00167-019-05552-w.
- Porter M, Shadbolt B, Ye X, Stuart R. Ankle lateral ligament augmentation versus the modified Broström‑Gould procedure: a 5‑year randomized controlled trial. Am J Sports Med. 2019;47(3):659‑666. doi:10.1177/0363546518820529.
- Kubick SE, Martinez AN, Mauren NR. Modified Broström vs suture tape augmentation: a systematic review. J Foot Ankle Surg. 2025;64(1):86‑90. doi:10.1053/j.jfas.2024.09.013.
- Cho BK, Park KJ, Park JK, SooHoo NF. Outcomes of the modified Broström procedure augmented with suture‑tape for ankle instability in patients with generalized ligamentous laxity. Foot Ankle Int. 2017;38(4):405‑411. doi:10.1177/1071100716683348.
- Scott RT, Doty JF, Philbin TM, et al. Evaluation of a biodegradable synthetic matrix for lateral ankle ligament surgical repair augmentation: an open label controlled multicenter retrospective review. Biomed J Sci Tech Res. 2024;56:008911. doi:10.26717/BJSTR.2024.56.008911