Table 1. A multimodal risk-stratified VTE prophylaxis protocol was prospectively evaluated in elective TJA patients.
Gregory A. Brown, MD, PhD, FAAOS
Published 5/28/2026
|
Gregory A. Brown, MD, PhD, FAAOS
Editor’s note: The following letter to the editor is in response to “Evidence-based guidelines needed for perioperative antithrombotic management in TJA,” by Theodor Di Pauli von Treuheim, MD; Benjamin Padon, BS; Anzar Sarfraz, MD; Garrett Ruff, BS; Vinay K. Aggarwal, MD; published in the August/September 2025 issue of AAOS Now.
A recent AAOS Now article rightly called for evidence-based guidelines for perioperative antithrombotic management (venous thromboembolism — VTE — prophylaxis) in total joint arthroplasty (TJA) that include patients with medical and bleeding risks. Risk-stratified protocols need both level I therapeutic evidence, such as randomized controlled trials (RCTs), and level I prognostic evidence (prospective, observational cohort studies). By definition, risk assessment requires prognostic evidence. The rationales and prognostic evidence for risk-stratified VTE prophylaxis protocols exist.
What we lack is a guideline development process that does not downgrade observational studies. AAOS uses a modified Grading of Recommendations, Assessment, Development and Evaluations (GRADE) methodology to develop clinical practice guidelines (CPGs). Prognostic evidence is initially downgraded to low-quality evidence. We need a new guideline development process that incorporates high-quality prognostic evidence for risk assessment.
Table 1. A multimodal risk-stratified VTE prophylaxis protocol was prospectively evaluated in elective TJA patients.
Gregory A. Brown, MD, PhD, FAAOS
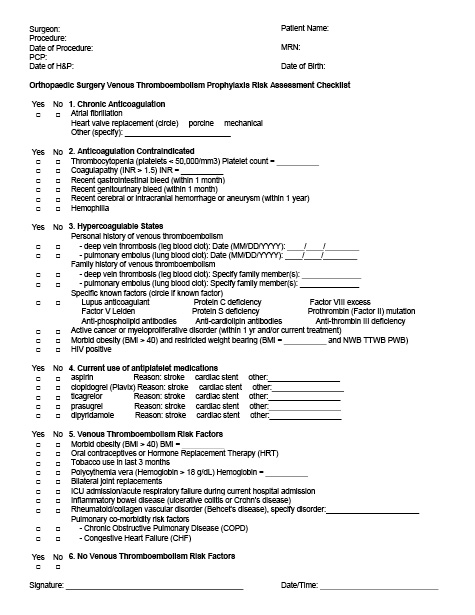
Table 2. A risk-stratified checklist was completed before surgery to determine the appropriate risk level.
Gregory A. Brown, MD, PhD, FAAOS
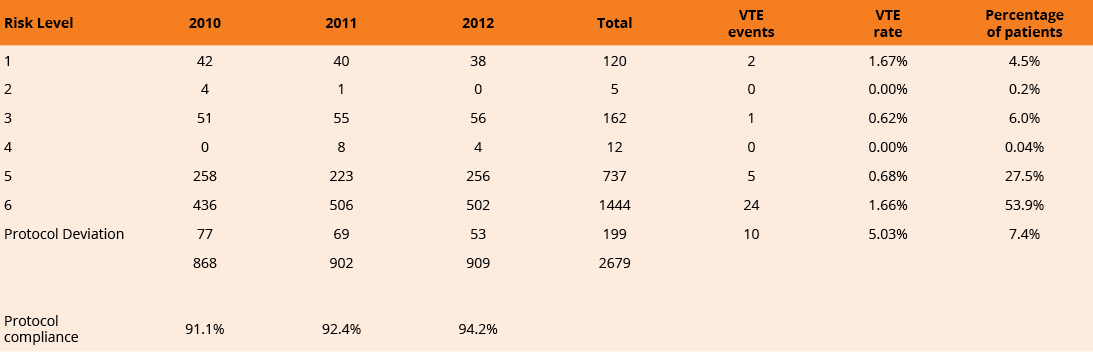
Table 3. Patients not following the protocol had a significantly higher VTE rate.
Gregory A. Brown, MD, PhD, FAAOS
Therapeutic and prognostic evidence are complementary
Therapeutic evidence and prognostic evidence serve distinct but complementary roles. Evidence-based medicine (EBM) was first defined as the combination of (1) the best available clinical evidence, (2) physician experience, and (3) patient preferences. RCTs are underpowered to perform subgroup analyses or detect differences in adverse events. VTE prophylaxis RCTs usually exclude patients on chronic anticoagulation, on antiplatelet therapy, or with a personal or family history of VTE. Large databases and registries are our collective experience and can provide robust estimates of prognostic factors and adverse events. Inclusion of prognostic evidence in guidelines would allow for individualized, evidence-based, shared decision making (SDM).
Limitations and bias in current guideline evidence
Bias can be introduced into RCTs and CPGs in many ways. Selecting a weak comparator favors the intervention. Low-molecular-weight heparin (LMWH) RCTs used warfarin as a weak comparator because warfarin is difficult to dose and requires frequent laboratory testing. Direct oral anticoagulants (DOACs) used LMWH as a weak comparator because LMWH has a high bleeding complication rate. The American College of Chest Physicians (ACCP) VTE prophylaxis guidelines used asymptomatic deep vein thromboses (DVTs) as the only measure of effectiveness and ignored symptomatic DVTs, pulmonary emboli (PEs), and fatal PEs. By requiring venography, the ACCP guidelines excluded the Pulmonary Embolism Prevention (PEP) trial comparing aspirin to placebo from the evidence base. Neither the ACCP guidelines nor the American Society of Hematology (ASH) VTE prophylaxis guideline includes adverse events, such as bleeding complications, in their recommendations.
Aspirin and anticoagulants: effectiveness depends on patient risk
Aspirin has been systematically excluded from pharmaceutical industry-funded TJA VTE prophylaxis RCTs. In spite of this exclusion, more recent CPGs include aspirin for VTE prophylaxis after TJA. The 2019 ASH guidelines recommend using aspirin or anticoagulants and recommend using DOACs over LMWH. Neither of these guidelines makes recommendations regarding patients with VTE, bleeding, or medical risks.
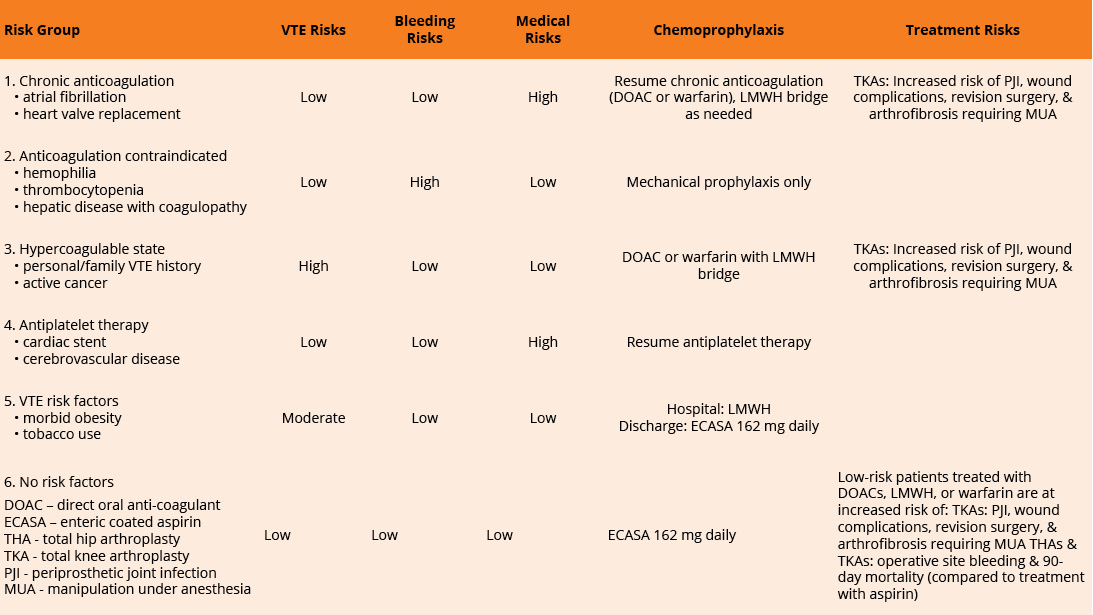
Once level I therapeutic evidence has confirmed the effectiveness of pharmacologic agents for VTE prophylaxis, prognostic evidence is needed to determine which agents are best for patients with VTE, bleeding, and/or medical risks. The medical risks of patients on chronic anticoagulation or antiplatelet therapy outweigh the VTE risks, so these patients should resume their chronic anticoagulation or antiplatelet therapy after TJA. VTE chemoprophylaxis increases bleeding, so patients with hemophilia, thrombocytopenia, or hepatic disease with coagulopathy should receive mechanical prophylaxis only. The optimal VTE chemoprophylaxis for patients with high, moderate, and low VTE risks can be determined with the best available prognostic and decision analyses evidence.
The only published VTE prophylaxis RCT including patients with a personal history of VTE is the CRISTAL trial, which compared aspirin to LMWH for patients undergoing TJA. A secondary analysis (not included in the study) of the VTE history subgroup shows patients treated with aspirin (23/270 = 8.5%) had a significantly higher rate of VTE events than those treated with LMWH (6/228 = 2.6%) (P = 0.0082, odds ratio = 3.45). The best available evidence suggests that aspirin should not be used for VTE prophylaxis in high-risk individuals. Other VTE high-risk patients are those with cancer or HIV.
For patients with no VTE risk factors (low risk), aspirin has a low rate of VTE events. An analysis of the Michigan Arthroplasty Registry Collaborative Quality Initiative (41,537 TKA patients) found the VTE rate for patients treated with aspirin alone was 1.16% (149/12,831) and for patients treated with anticoagulation alone was 1.42% (321/22,620). A meta-analysis comparing aspirin to anticoagulants (LMWH, warfarin, DOACs) found that aspirin was non-inferior and cost-effective for VTE prophylaxis after TJA. For patients treated with aspirin, the relative risk of DVT was 1.04 (95% CI 0.72-2.51) and the relative risk of PE was 1.01 (95% CI 0.68-1.48). A cost-utility analysis of THA patients found that aspirin was cost-effective for patients with no history of VTE.
Chemoprophylaxis risks need to be included in recommendations
A pooled analysis of RCTs cited in the ACCP guidelines showed that LMWH and warfarin had significantly higher operative site bleeding rates than aspirin, and DOAC bleeding risks are comparable to LMWH risks. TKA patients receiving LMWH, warfarin, or DOACs are at increased risk of arthrofibrosis requiring manipulation under anesthesia, periprosthetic joint infection, sepsis, hematoma, wound dehiscence, and all-cause revision surgery. TJA patients receiving LMWH, DOACs, or warfarin had increased rates of mortality and symptomatic nonfatal pulmonary emboli compared to aspirin.
Observational evidence informs duration of prophylaxis
The duration of VTE prophylaxis can be guided by observational evidence. An observational cohort of 947,454 women in the United Kingdom (Million Women Study) was prospectively monitored for postoperative venous thromboembolism. During follow-up, 239,614 women had surgery. For the hip and knee replacement subgroup, the relative risks for VTE after surgery were 220.6 (187.8-259.2), 39.7 (27.3-57.8), 4.6 (2.9-7.2), and 2.7 (1.9-4.0) at zero to six weeks, seven to 12 weeks, four to 12 months, and greater than one year, respectively. VTE prophylaxis after TJA surgery should continue for at least 90 days.
Prospective evaluation of a risk stratified multimodal protocol
A multimodal risk-stratified VTE prophylaxis protocol was prospectively evaluated in elective TJA patients (Table 1). In addition to chemoprophylaxis, patients received early mobilization, inpatient mechanical prophylaxis, and neuraxial anesthesia (preferred). VTE prophylaxis was continued for 90 days. A risk-stratified checklist was completed before surgery to determine the appropriate risk level (Table 2). Compared with the year before protocol implementation, the 90-day VTE rate decreased from 3.40% (38/1118) to 1.57% (42/2679), P = 0.0007. TKA procedures had twice the VTE rate as THA procedures, 2.00% (32/1604) versus 0.93% (10/1075), respectively, P = 0.0379. Patients not following the protocol had a significantly higher VTE rate, 5.03% versus 1.29%, respectively (P = 0.0007; odds ratio = 4.05, P = 0.0002; Table 3). This odds ratio is remarkably close to the OR in the CRISTAL trial for patients with a history of VTE. This prospective observational cohort provides Level I prognostic evidence that a risk-stratified VTE prophylaxis protocol for TJA patients reduces the VTE risk of patients at high-risk for VTE.
Clinical practice guidelines need to be restructured to include prognostic evidence and adverse events/harms. CPGs should summarize the best available evidence for all important patient questions. Table 1 can be used as a decision aid for TJA VTE prophylaxis SDM.
Gregory A. Brown, MD, PhD, FAAOS, was a member of the AAOS Guidelines Oversight Committee from 2010-2014. He was sub-chair for the AAOS Clinical Practice Guidelines on the Evidence-Based Quality and Value Committee from 2016-2018.
References
- Di Pauli von Treuheim T, Padon B, Sarfraz A, Ruff G, Aggarwal VK. Evidence-based guidelines needed for perioperative antithrombotic management in TJA. AAOS Now 2025-August September 2025. www.aaos.org/aaosnow/2025/aug-sept/clinical/clinical04/
- Wright JG, Swiontkowski MF, Heckman JD. Introducing levels of evidence to the journal. J Bone Joint Surg Am. 2003;85(1):1-3.
- BMJ Best Practice. What is GRADE? https://bestpractice.bmj.com/info/us/toolkit/learn-ebm/what-is-grade/. Accessed April 20, 2026.
- Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn't. BMJ 1996;312(7023):71-72.
- Goldacre B. Bad Pharma: How Drug Companies Mislead Doctors and Harm Patients. New York, NY: Faber and Faber; 2012.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(3 Suppl):338S-400S.
- Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):381S-453S.
- Prevention of pulmonary embolism and deep vein thrombosis with low-dose aspirin: Pulmonary Embolism Prevention (PEP) trial. Lancet. 2000;355(9212):1295-1302.
- Guyatt GH, Akl EA, Crowther M, et al. Executive summary: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):7S-47S.
- Anderson DR, Morgano GP, Bennett C, et al. American Society of Hematology 2019 guidelines for management of venous thromboembolism: prevention of venous thromboembolism in surgical hospitalized patients. Blood Adv. 2019;3(23):3898-3944.
- Group CS, Sidhu VS, Kelly TL, et al. Effect of aspirin vs enoxaparin on 90-day mortality in patients undergoing hip or knee arthroplasty: a secondary analysis of the CRISTAL cluster randomized trial. JAMA Netw Open. 2023;6(6):e2317838.
- Farge D, Frere C, Connors JM, et al. 2022 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer, including patients with COVID-19. Lancet Oncol. 2022;23(7):e334-e347.
- Olson JJ, Schwab PE, Jackson J, Lange JK, Bedair HS, Abdeen A. HIV-positive patients are at increased risk of venous thromboembolism after total joint replacement. J Am Acad Orthop Surg. 2021;29(11) :479-85.
- Hood BR, Cowen ME, Zheng HT, Hughes RE, Singal B, Hallstrom BR. Association of aspirin with prevention of venous thromboembolism in patients after total knee arthroplasty compared with other anticoagulants: a noninferiority analysis. JAMA Surg. 2019;154(1) :65-72.
- Matharu GS, Kunutsor SK, Judge A, Blom AW, Whitehouse MR. Clinical effectiveness and safety of aspirin for venous thromboembolism prophylaxis after total hip and knee replacement: a systematic review and meta-analysis of randomized clinical trials. JAMA Intern Med. 2020;180(3):376-384.
- Schousboe JT, Brown GA. Cost-effectiveness of low-molecular-weight heparin compared with aspirin for prophylaxis against venous thromboembolism after total joint arthroplasty. J Bone Joint Surg Am. 2013;95(14) :1256-1264.
- Brown GA. First Annual American Association of Hip and Knee Surgeons Clinical Award - venous thromboembolism prophylaxis after major orthopaedic surgery: a pooled analysis of randomized controlled trials. J Arthroplasty. 2009;24(6 Suppl) :77-83.
- Russell RD, Huo MH. Apixaban and rivaroxaban decrease deep venous thrombosis but not other complications after total hip and total knee arthroplasty. J Arthroplasty. 2013;28(9):1477-1481.
- Johnson AH, Brennan JC, Simpson SS, Turcotte JJ, King PJ. The effect of chronic anticoagulation on early postoperative outcomes following total knee arthroplasty: A TriNetX database study. Arthroplast Today. 2025;33:101690.
- Anil U, Kirschner N, Teo GM, et al. Aspirin thromboprophylaxis following primary total knee arthroplasty is associated with a lower rate of early prosthetic joint infection compared with other agents. J Arthroplasty. 2023;38(6 Suppl):S345-S349.
- Goel RK, Ross BJ, Heo KY, et al. Chronic anticoagulation is associated with significantly increased rates of medical complications, periprosthetic joint infection, and revision after primary total knee arthroplasty. Arthroplast Today. 2025;34:101749.
- Sharrock NE, Gonzalez Della Valle A, Go G, Lyman S, Salvati EA. Potent anticoagulants are associated with a higher all-cause mortality rate after hip and knee arthroplasty. Clin Orthop Relat Res. 2008;466(3):714-721.
- Sweetland S, Green J, Liu B, et al. Duration and magnitude of the postoperative risk of venous thromboembolism in middle aged women: prospective cohort study. BMJ. 2009;339:b4583.
- Brown GA. Orthopaedic Education and Research Foundation/Current Concepts in Joint Replacement Clinical Practice Award - optimizing venous thromboembolism prophylaxis after total joint arthroplasty: a risk-stratified multi-modal VTE prophylaxis protocol reduces 30 day all-cause re-admissions and 90 day venous thromboembolic events. Presented at: Current Concepts in Joint Replacement; 2014; Las Vegas, NV.