Figure 1: Pain Management
*denotes significance p<0.05
*denotes significance p<0.05
Courtesy of the study authors
Published 5/28/2026
|
Theresa Witham
Although nonopioid pain control after trapeziectomy has been explored, there are still no established guidelines for managing pain in this patient population. A team of researchers conducted a randomized controlled trial to assess the efficacy of ibuprofen and acetaminophen combination compared to oxycodone for pain management in the first 30 days following trapeziectomy for carpometacarpal osteoarthritis, and they shared the results at the AAOS 2026 Annual Meeting in March.
Figure 1: Pain Management
*denotes significance p<0.05
*denotes significance p<0.05
Courtesy of the study authors
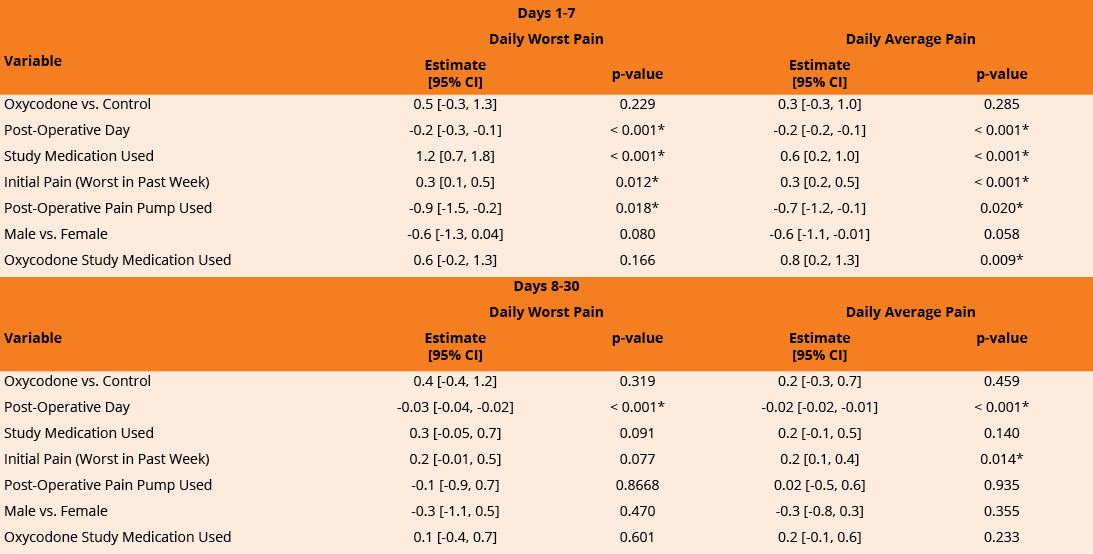
Figure 2: Adjusted Multivariable Models for Daily Worst and Average Pain Scores
*denotes significance p<0.05
*denotes significance p<0.05
Courtesy of the study authors
The investigators carried out an Institutional Review Board-approved double-blind randomized controlled trial, enrolling preoperative trapeziectomy patients from two academic institutions and a Veterans Affairs hospital from February 2021 to May 2025. Patients were randomized to receive 20 doses of either a 400 mg ibuprofen and 500 mg acetaminophen combination or 5 mg of oxycodone for postoperative pain control. All patients also received standardized nerve blocks, optional pain pumps, and four 5 mg oxycodone tablets for breakthrough pain not adequately controlled by the assigned study medication.
Numeric Pain Rating Scale (NPRS) scores out of 10 were used to record participants’ worst and average daily pain for postoperative days 1-30 via text messaging in REDCap. Outcomes were evaluated using bivariate comparisons and linear mixed effects models.
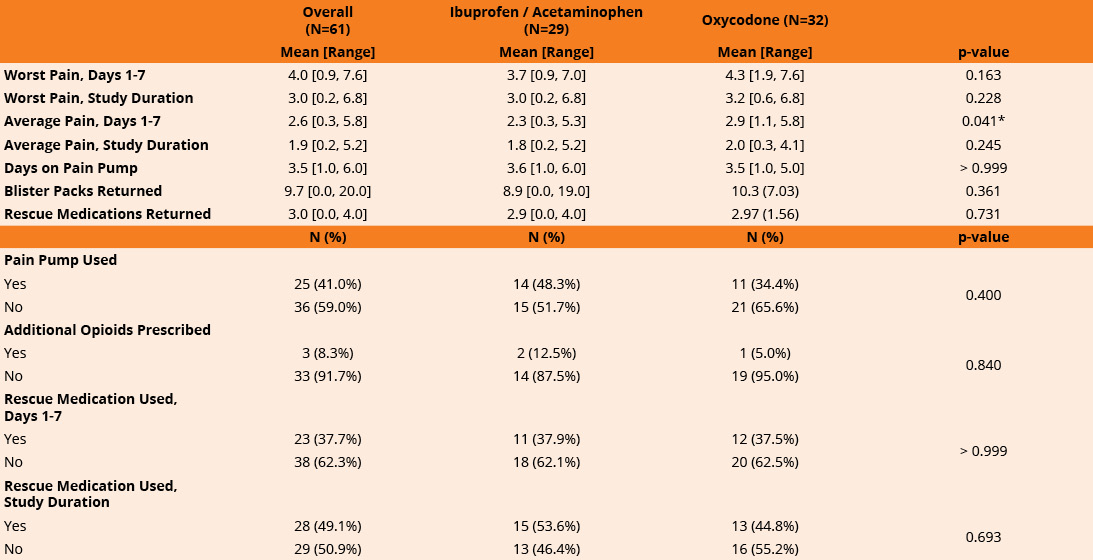
In this 61-patient study, 29 were randomized to the ibuprofen and acetaminophen combination, 38 (62.3%) were female, and 34 (55.7%) had surgery on their dominant hand. Those assigned to oxycodone reported slightly higher pain scores during the first postoperative week compared with patients receiving ibuprofen and acetaminophen (2.9/10 vs. 2.3/10). The study reported pain outcomes aggregated over postoperative days 1-7 and did not provide separate analyses for individual early postoperative days, such as days 1-2. The worst pain was noted during days 1-7, with a mean of 3.7/10 for the ibuprofen and acetaminophen group and a mean of 4.3/10 for the oxycodone group.
A total of 23 patients (about 40%) used the rescue medication in the first seven days after surgery, 11 from the ibuprofen/acetaminophen group and 12 from the oxycodone group. In total, 28 patients (46%) used the rescue medication during the study, 15 from the ibuprofen/acetaminophen group and 13 from the oxycodone group (Figure 1).
Adjusted analyses showed no meaningful differences in pain levels between the oxycodone group and the ibuprofen/acetaminophen group across the full 30‑day recovery period. During postoperative days 1-7, higher reported pain was associated with being earlier in the postoperative course, having higher baseline pain, not using a pain pump, and days on which patients took study medication, likely reflecting use of medication in response to increased pain (Figure 2).
For days 8-30, pain was similarly higher on days closer to surgery and in patients with higher baseline pain. Although patients in the oxycodone group used fewer study pills after postoperative day 1 and continued to do so through day 14, this pattern did not reflect superior pain control, as overall pain scores between groups remained comparable throughout the study period.
The authors noted several limitations, including that this is an interim analysis with a limited sample size, meaning results may shift as enrollment continues. They also acknowledged potential unblinding and the use of study-provided rescue oxycodone, as well as a small number of additional opioid prescriptions beyond the study protocol, which could have introduced bias in both medication use and reported pain.
“Our double-blind randomized controlled trial demonstrates that a ibuprofen and acetaminophen combination may provide effective pain control following trapeziectomy, as patients did not have significantly different pain scores in the first 30 days postoperative,” the authors wrote. “These findings may shape national guidelines to promote effective postoperative pain management following trapeziectomy while also minimizing unnecessary risks associated with opioids.”
This study was partially supported by an AFSH 2020 Two-year Clinical Grant, “Pain Relief after Trapeziectomy without Opioids: Ibuprofen & Acetaminophen versus Oxycodone.” Additional funding from the Williams Foundation helped provide essential personnel support.
The authors of “Pain relief after trapeziectomy: What a double-blind‑ study reveals about opioid vs. non‑opioid care” are Gabriella B. Smith, BA; Ashley L. Titan, MD; Deborah E. Kenney, MS, OTR/L; Nicole S. Pham, MPH; Tara Shelby, MD; Robert Reitz, MD; Angela Wang, MD, FAAOS; Paige M. Fox, MD, PhD; Jeffrey Yao, MD, FAAOS; and Amy L. Ladd, MD, FAAOS.
Theresa Witham is managing editor for AAOS Now.