Published 2/27/2026
|
Leslie Schwindel, MD, FAAOS
Enhanced Recovery After Surgery (ERAS) is a multimodal perioperative care pathway/protocol designed to achieve early recovery and reduce hospital stays for patients undergoing major surgery. It was initiated by the ERAS Society, an international, professional nonprofit organization founded in 2010. The ERAS pathway is patient-centered, multimodal, and multidisciplinary and claims to be able to shorten recovery time and complication rates by 30% or more.
The key factors that keep patients in the hospital after surgery include the need for parenteral analgesia, the need for IV fluids secondary to gut dysfunction, and bed rest caused by lack of mobility. The central elements of the ERAS pathway address these key factors, helping to clarify how they interact to affect patient recovery. Protocols have been developed for multiple specialties, including rectal, urological, bariatric surgery, and total hip and knee arthroplasty (THA, TKA). The main principles of an orthopaedic ERAS pathway can be divided into four stages: prehospital, preoperative/day of surgery, intraoperative, and postoperative.
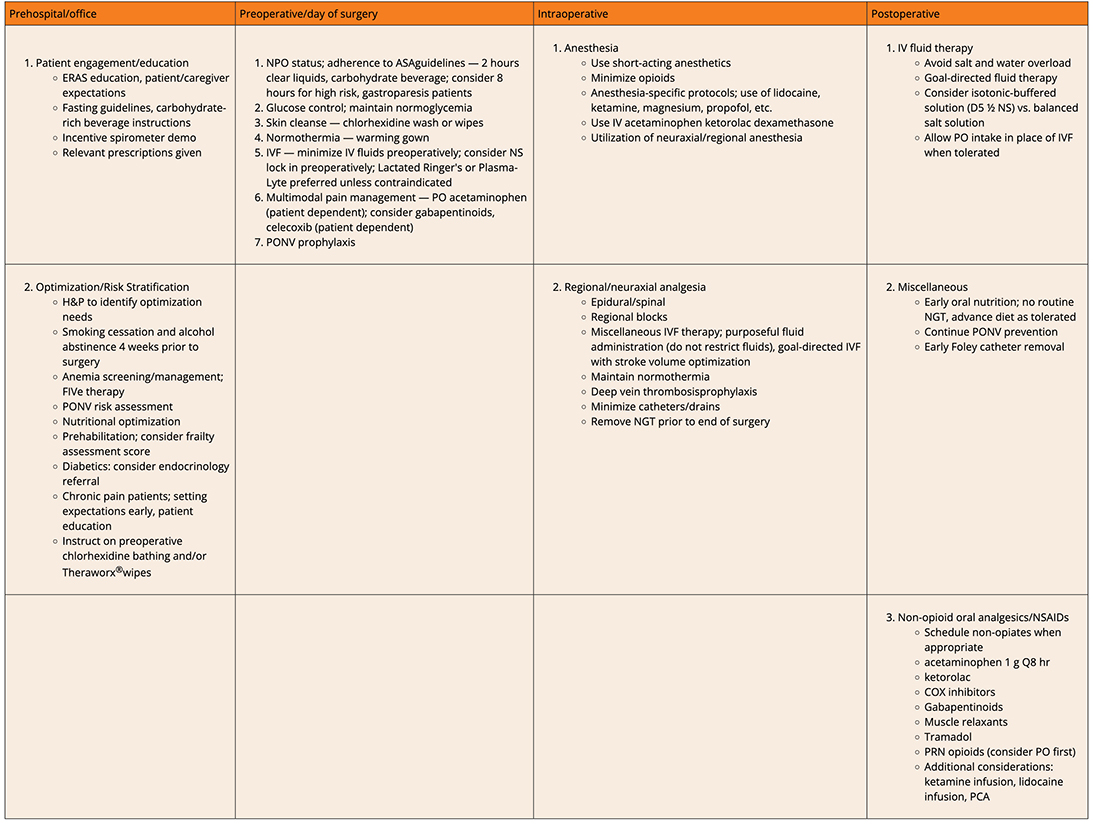
Table 1: The Four Stages of ERAS
FIVe therapy, folate, iron, vitamin B12/C and/or erythropoietin; PONV, Postoperative nausea/vomiting; NGT, nasogastric tube
FIVe therapy, folate, iron, vitamin B12/C and/or erythropoietin; PONV, Postoperative nausea/vomiting; NGT, nasogastric tube
Prehospital focus is on optimization of preoperative physical/psychological factors, such as identification and management of anemia, malnutrition, and suboptimal glucose control. Patient education is emphasized, and discharge planning arrangements are planned.
Day of surgery/intraoperative factors considered are atraumatic surgical techniques, standardized anesthesia/analgesia protocols, multimodal opioid sparing analgesia regimens, and promotion of normovolemia, normothermia, and prevention of hypoxia.
Postoperatively, early ambulation with effective analgesia is essential, avoiding opioids where feasible. Catheters, drains, and drips are not used or are removed as soon as possible; patients are encouraged to eat and drink early and wash/dress/socialize as soon as possible. All patients are discharged home using agreed criteria managed by the multidisciplinary team, with clear instructions and support or progressing independently. These principles are summarized in Table 1 below.
The first orthopaedic surgeries to use enhanced recovery pathways were total hip and knee arthroplasty. These procedures were chosen as they were high volume, had long hospital length of stays, and carried high costs. Enhanced recovery pathways were first widely adopted in countries such as Denmark and the U.K. Their success led to international adoption, and enhanced recovery is now broadly accepted as best practice for hip and knee arthroplasty surgeries. Reports suggest a decrease in length of hospital stay after total hip and knee arthroplasty from four to 12 days to one to three days with no significant increase in readmission for any reason as a result of implementing the ERAS protocol.
A consensus statement was released by the ERAS Society in 2020 regarding perioperative care in total hip and knee replacement. The group graded the following recommendations as “Strong”:
- Patients should routinely receive preoperative education.
- Smoking/alcohol should stop four weeks preoperatively; anemia screening/treatment is recommended early.
- Preoperative fasting: Clear fluids should be allowed up to two hours and solids up to six hours prior to induction of anesthesia.
- General anesthesia and neuraxial techniques may both be used as part of multimodal anesthetic regimes.
- Within a multimodal opioid-sparing analgesic regimen, the routine use of local infiltration analgesia (LIA) is recommended for TKA but not THA. Nerve block techniques have not shown clinical superiority over LIA.
- Patients should be screened for and given multimodal PONV prophylaxis/treatment.
- Tranexamic acid (TXA) is recommended to reduce perioperative blood loss and the requirement for transfusion.
- A multimodal opioid-sparing approach to analgesia should be adopted. The routine use of paracetamol/acetaminophen and NSAIDs is recommended for patients without contraindications.
- Normal body temperature should be maintained peri- and postoperatively.
- Patients should receive systemic antimicrobial prophylaxis.
- Patients are at increased risk of venous thromboembolism and should undergo pharmacologic and mechanical prophylaxis in line with local policy.
- There is no conclusive evidence that the choice of surgical approach accelerates the achievement of discharge criteria.
- Fluid balance should be maintained to avoid over- and under-hydration.
- An early return to a normal diet should be promoted.
- Patients should be mobilized as early as they are able to facilitate early achievement of discharge criteria.
- Team-based functional discharge criteria should be used to facilitate patient discharge directly to their home.
The implementation of ERAS protocols represents a transformative shift in orthopaedic surgery. Its strength lies not in any single intervention but in the coordinated, patient-centered efforts of the entire surgical team. By systematically addressing the physiological stressors of major surgery through a four-stage multidisciplinary approach, these pathways have proven their capacity to reduce complications, shorten hospital stays, and improve overall patient satisfaction. Through early mobilization, effective non-opioid analgesia, and proactive preoperative optimization, surgeons can significantly accelerate a patient's return to their daily life. Further efforts to refine and audit these protocols will be essential to maintaining high standards of care, ensuring that every patient benefits from a safer, faster, and more satisfying surgical experience.
Leslie Schwindel, MD, FAAOS, is a board-certified general orthopaedic surgeon at Lake Cumberland Regional Hospital in Somerset, Kentucky. She is also a member of the AAOS Now Editorial Board.
References
- ERAS® Society. Home - ERAS® Society. erassociety.org/. Accessed February 11, 2026.
- Wainwright TW, Gill M, McDonald DA, Middleton RG, Reed M, Sahota O, Yates P, Ljungqvist O.
Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations.
Acta Orthop. 2020;91(1):3-19. - American Association of Nurse Anesthesiology. Enhanced Recovery After Surgery.
www.aana.com/practice/clinical-practice/clinical-practice-resources/enhanced-recovery-after-surgery/.
Accessed February 11, 2026. - Williams DGA, Wischmeyer PE. Perioperative Nutrition Care of Orthopedic Surgery Patient. Tech Orthop. 2020;35(1):15-18. doi:10.1097/bto.0000000000000412