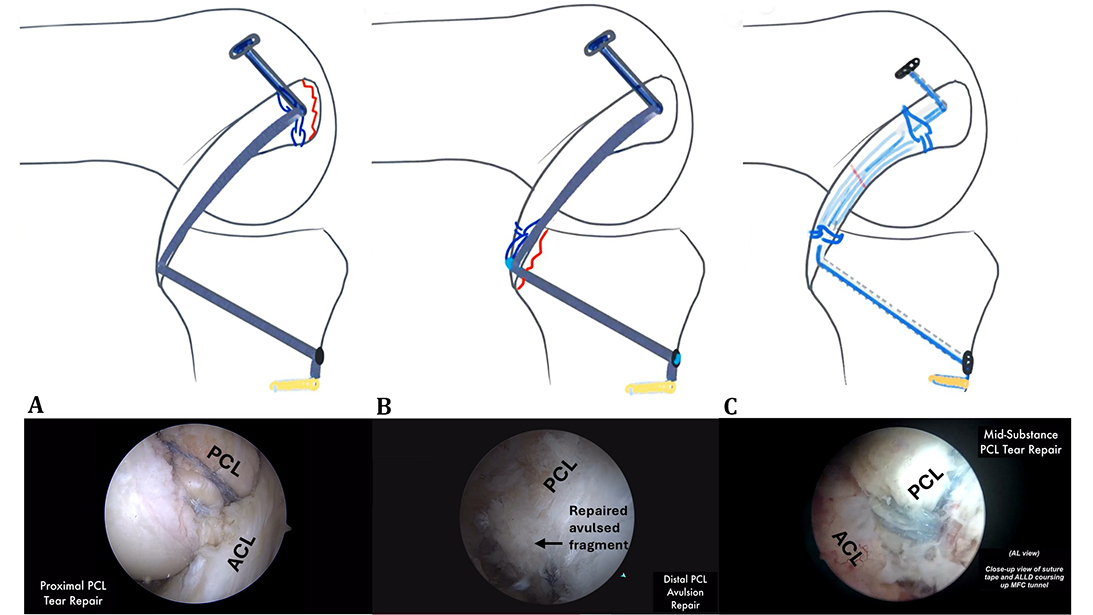
Figure 1. Diagram of the repair construct and arthroscopic images of PCL primary repairs for proximal tears (A), distal avulsions (B), and mid-substance tears (C).
Published 2/27/2026
|
Richard Ma, MD, FAAOS
Editor's note: The following article is a review of a video available via the AAOS Orthopaedic Video Theater (OVT). AAOS Now will routinely review “OVT Plus” videos, which are vetted by topic experts and offer CME. For more information, visit aaos.org/OVT.
Posterior cruciate ligament (PCL) injuries are uncommon knee injuries. The standard treatment for most isolated PCL tears is unclear. Studies have shown that low-grade to mid-grade PCL injuries may heal satisfactorily with nonoperative treatment, including with bracing and rehabilitation. In comparison, high-grade injuries may warrant surgical repair, particularly in high-level athletes or in injuries where other knee ligaments are involved.
In the AAOS OVT video titled “Arthroscopic Repair of Midsubstance Posterior Cruciate Ligament Tears,” Jim Hsu, MD, FAAOS, noted that part of the treatment challenge with PCL injuries is the long recovery and mixed outcomes, including residual laxity with both conservative treatment and PCL reconstructions with grafts. Recently, interest in primary PCL repair has gained interest, in part due to advancements in arthroscopic technique and instrumentation that have made primary repair technically easier to accomplish. Some advantages of PCL repair noted by Dr. Hsu include harnessing the PCL's native ability to heal, restoring native ligament tension to potentially reduce final knee laxity, and using a more minimally invasive approach relative to standard reconstruction techniques.
The OVT video highlighted how an MRI imaging study found that most PCL injuries occur mid-substance (69%) versus its proximal attachment (27%) or distal avulsion (9%). The development and combination of tensionable knotless endobutton systems that can be assembled intraoperatively, better grasping suture technology (a high-strength, pre-looped, suture-based fixation device) to capture the residual native PCL and shuttle repair sutures to incorporate them into the endobutton systems, and synthetic suture tapes for bracing the primary PCL repairs have made repairs of PCL tears technically feasible and reproducible.
Dr. Hsu outlined his broad approaches to PCL repair in four steps:
- capturing the residual native injured PCL with the pre-looped suture fixation device;
- loading the pre-looped sutures onto a tensionable endobutton system that can be assembled on the surgical field;
- passing and securing the internal brace suture tape across the PCL through the endobutton on the femur and suture anchor on the tibia, respectively; and
- tensioning the native PCL repair via the endobutton system.
In the OVT video, the author outlined a combination of these key steps for primary repair of PCL proximal tears, distal avulsions, and, finally, the mid-substance tears.
For proximal PCL tears, two pre-looped suture devices are used to capture the residual PCL stump with a standard self-retrieving suture passing device often used for rotator cuff repairs. A 3.0 mm tunnel is then drilled into the native PCL femoral footprint, and a passing suture is then placed across the femoral 3.0 mm tunnel. Two additional pre-looped sutures are used to shuttle the limbs of the endobutton system, which is then assembled on the field, incorporating the two pre-looped sutures grasping the native PCL stump. Once assembled, the endobutton and the suture tape (for bracing the primary repair) are passed through the 3.0 mm tunnel and docked into place on the lateral aspect of the femur. The PCL tibial tunnel is then established in the posterior tibia with a PCL tibial drill guide. A cannulated drill bit is used to drill from the anteromedial tibia up to the PCL tibial footprint, and a guide wire is passed through the cannulation within the cannulated drill bit. The tibial end of the suture tape is then passed and fixed into a suture anchor on the tibia, with the knee at 90 degrees and an anterior drawer to reduce the tibia. Final tension is then applied on the femoral side of the endobutton to achieve the final fixation of the PCL primary repair.
Dr. Hsu noted that PCL distal avulsions often occur with a bony fragment. A novel two-endobutton construct (one on the femur and one on the tibia) is used to repair a distal avulsion. Like proximal avulsion repair, the procedure begins with two pre-looped sutures used to capture the distal PCL, just proximal to the avulsed bony fragment. Two additional pre-looped sutures are used to shuttle the limbs of the endobutton system to incorporate the pre-looped sutures grasping the native PCL, which is then assembled on the surgical field. The tibial tunnel is then established, followed by the femoral tunnel, implemented with a similar technique as the proximal repairs, with two corresponding shuttling wires for passage in the tibia and one shuttling wire in the femoral tunnel. The ends of the two pre-looped sutures grasping the distal segment of the PCL are then passed through the tibia with one set of shuttling wire. A second endobutton system with the suture tape for bracing the primary repair is passed with the button in an outside-in fashion through the femoral tunnel, followed by passage through the tibial tunnel. The bony fragment is reduced arthroscopically, and the ligament bracing with the suture tape is completed with a suture anchor and application of an anterior drawer with the knee at 90 degrees. Finally, a suture button-style endobutton is assembled on the tibial side, and the endobutton is tensioned, completing the distal avulsion repair.
The author ended the OVT video with a novel technique for mid-substance PCL repairs. This is a more complex repair, as two sets of two pre-looped sutures are placed in the proximal and distal end of the mid-substance PCL tear, which are then threaded through the opposing segment of the PCL and incorporated into a respective endobutton system (e.g., proximal PCL segment incorporated into the tibial endobutton and vice versa). A suture tape is also incorporated into the repair construct. Two posteromedial portals are needed, and meticulous suture management is critical for this technique.
Dr. Hsu followed the technique video with a discussion of a cadaveric biomechanical study showing equivalent posterior displacement (134N load) with the novel mid-substance repair with internal brace (2.98 ± 0.37 mm) versus intact PCL states (3.34 ± 0.97 mm). The author also noted positive functional outcomes with return to different activities in a small limited clinical series at two years after surgery.
Overall, this OVT video highlights the potential role for primary PCL repair in the surgical treatment algorithm for PCL injuries. It provides technical strategies to achieve a primary PCL repair to address proximal, distal, and mid-substance tears using modern arthroscopic instrumentation and technique. It therefore has educational value for surgeons who may be evaluating the evidence and technique for PCL primary repair.
Richard Ma, MD, FAAOS, is the Gregory L. and Ann L. Hummel Distinguished Professor and Director of Sports Medicine in the Department of Orthopaedic Surgery at the University of Missouri. He also serves as a member of the AAOS Now Editorial Board.
References
- Suneja A, Deshpande SV, Wamborikar H, Date SV, Goel S, Sekhon G. Outcome analysis of posterior cruciate ligament injuries: A narrative review. Cureus. 2023;15(10):e47410. doi:10.7759/cureus.47410
- Farshad-Amacker NA, Potter HG. MRI of knee ligament injury and reconstruction. J Magn Reson Imaging. 2013;38(4):757-773. doi:10.1002/jmri.24311
Video Details
Title: Arthroscopic Repair of Midsubstance Posterior Cruciate Ligament Tears
Authors: Jim C. Hsu, MD, FAAOS; Nancy Park, BS; Soheil Sabzevari, MD; Serkan Surucu, MD
Published: March 1, 2025
Time: 22:18
Tags: Sports Medicine, Knee Ligament Injuries, Reconstruction
Visit aaos.org/OVT to view this title and more than 1,600 other videos from across orthopaedic topics, institutions, practice management, and industry.