
Figure 1. Sunset over Lubango, Angola
Courtesy of Douglas W. Lundy, MD, MBA, FAAOS
Published 2/27/2026
|
Douglas W. Lundy, MD, MBA, FAAOS, FACS; Michael J. DeRogatis, MD, MS; Annelise F. Olson, MD, FACS
The January 2025 AAOS Now article titled “Douglas W. Lundy, MD, MBA, Shares Highlights, Key Lessons from Recent Orthopaedic Mission Trip to Angola,” described a 2024 short-term mission trip to Lubango, Angola, a middle-income country in Africa whose official language is Portuguese. That trip introduced total knee arthroplasty (TKA) to full-time Angolan missionary surgeons as a first step in a sustainable program to help patients with severe knee arthritis in southwestern rural Africa. More than half the surgical volume of the general surgeons at Centro Evangélico de Medicina do Lubango (CEML) is orthopaedic surgery, including total hip arthroplasty (THA). The team recently returned to CEML to further develop the TKA program.
One of the common criticisms of short-term medical missions by North American physicians is that the care provided in these endeavors is often unsustainable, and surgical complications can severely compromise affected patients' ability to cope after well-meaning surgeons return home. Enthusiastic surgical teams from the United States altruistically give their time and energy to travel into the developing world and deliver high-quality care to suffering people. In many cases, however, the local surgical teams do not gain any education and training from these experiences, and these short bursts of care cannot be sustained. As a result, small numbers of people are helped, complications are not addressed, and the overall health of the community is not materially improved.
Figure 1. Sunset over Lubango, Angola
Courtesy of Douglas W. Lundy, MD, MBA, FAAOS

Figure 2. AP radiograph after total knee arthroplasty
Courtesy of Douglas W. Lundy, MD, MBA, FAAOS

Figure 3. Surgical team performing total knee arthroplasty
Courtesy of Douglas W. Lundy, MD, MBA, FAAOS

Figure 4. Surgical team performing tibial osteotomy and distraction osteogenesis
Courtesy of Douglas W. Lundy, MD, MBA, FAAOS
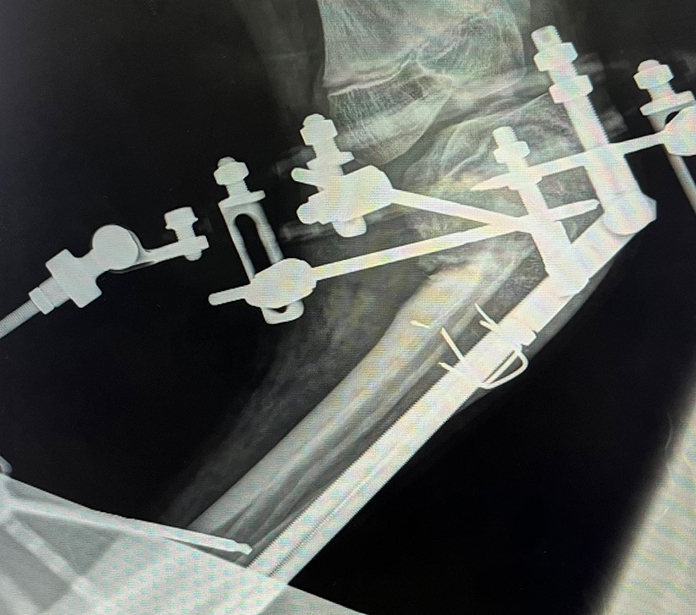
Figure 5. Post-operative AP radiograph after tibial osteotomy
Courtesy of Douglas W. Lundy, MD, MBA, FAAOS

Figure 6. AP radiograph demonstrating progressive correction of tibial deformity
Images Courtesy of Douglas W. Lundy, MD, MBA, FAAOS
Complications after orthopaedic surgery can be extremely debilitating even in the most advanced settings, and these situations are even more magnified in resource-challenged locales. The severity of the pathology that presents in the developing world is often far more severe than is routinely seen in the United States, and the complications that present after treatment of these conditions can be equally challenging. A reasonable philosophical question persists: “Would patients be better off without 'first world' surgery than risk catastrophic complications with absolutely no chance of cure?”
Another issue is the belief that general surgeons can be quickly trained to perform one of the more challenging procedures in elective orthopaedic surgery. Total joint arthroplasty (TJA) is arguably one of the more complicated procedures that orthopaedic surgeons perform, and imparting required training to general surgeons over two separate week-long trips seems unreasonable. In addition, the severity of the arthritis and the requisite deformities that these surgeons treat are among the most challenging cases that even expert reconstructive surgeons face. Since patients in the most resource-deficient areas of the world have little to no access to modern care, their disease patterns progress to an extent rarely seen in the United States. As a result, it is not uncommon for general surgeons working with limited resources to consider complex procedures to relieve the suffering of the patients they encounter. It is important to realize that general surgeons working in the developing world differ from the general surgeons in the U.S. healthcare systems. In resource-challenged locations, much of these surgeons' workload is within the musculoskeletal system.
The dilemma is whether we should encourage the development of complex surgical programs in these settings, knowing that the severity of disease would challenge even top experts in the United States, yet recognizing that these patients suffer just to survive. Is it acceptable to undertake these procedures in a suboptimal environment with limited options, all in the name of empathic care? Or is it better to encourage the surgeons to stay within the bounds of safer procedures and avoid the potential complications that are bound to occur in these complex patients? Every introspective surgeon who participates in one of these trips must deliberate this ethical quandary.
The visiting team worked exclusively with the attending local surgeons and residents, teaching the principles and techniques of TKA as well as other procedures. Integral to this instruction were the principles of selecting the correct surgical candidates and including recognition of patient pathology beyond the capabilities of the environment. As time progressed, the team gradually disengaged from the teaching process, allowing the local surgeons to “fly on their own” while still providing extensive real-time feedback. The surgical techniques used were appropriate in the setting, and education also included the local surgical nurses, technicians, and support personnel. Language barriers added a layer of complexity, as only the surgeons and residents spoke English, and none of the visiting team spoke Portuguese.
As a fellowship-trained trauma surgeon, the senior surgeon on the trip (Dr. Lundy) contributed by addressing complex trauma cases presenting with deformity, infections and nonunions, which far surpass the pathologies usually encountered in the United States.
Sustainable arthroplasty depends on implant access and local commitment
One of the main obstacles in developing an arthroplasty program in resource-challenged countries is the sustainable availability of implants. Finding inexpensive components that would remain available for the foreseeable future was critical to the project. Local surgeons might struggle to keep up with the different techniques and specific implant nuances if cost demanded switching between implant manufacturers. The local host, Annelise Olson, MD, was able to identify an inexpensive implant source anticipated to support the arthroplasty program in CEML for quite a while. Though far less expensive than the implants used in the United States, these components are of good quality, and the tibial inserts are composed of ultra-high molecular weight polyethylene.
The team found working in the developing world to be an extremely rewarding experience. The privilege of delivering care to those with no other option and supporting local surgeons in providing sustainable future care created an existential sense of meaning. These experiences are certainly not for everyone, and surgeons considering working in the developing world should first travel with a team experienced in these settings. Although the team plans to return to Angola, recruiting fellowship-trained orthopaedic surgeons for these short-term trips remains a challenge.
In the meantime, the team continues to virtually mentor the Angolan surgeons and help them with case preparation and feedback after surgery. WhatsApp is extremely helpful in this regard, and electronic video chats are extremely easy once you get around the time zone differences (Angola is six hours ahead of Eastern Time). The capacity to be flexible and understand the limits of what can be safely accomplished is integral to success. Establishing reasonable goals, although often short of the perfection sought in the United States, will provide substantial relief to many suffering from orthopaedic conditions in the most remote settings.
Douglas W. Lundy, MD, MBA, FACS, FAAOS, is chair of orthopaedic surgery and chief of orthopaedic trauma surgery at St. Luke's University Health Network, in Bethlehem, Pennsylvania. He is also the deputy editor of AAOS Now and a member of the AAOS Now Editorial Board.
Michael DeRogatis, MD, MS, is an orthopaedic surgery resident at St. Luke's University Health Network in Bethlehem, Pennsylvania, and serves as a resident member of the AAOS Now Editorial Board.
Annelise F. Olson, MD, FACS, is a general surgeon and director of surgery at Centro Evangélico de Medicina do Lubango, in Lubango, Angola.