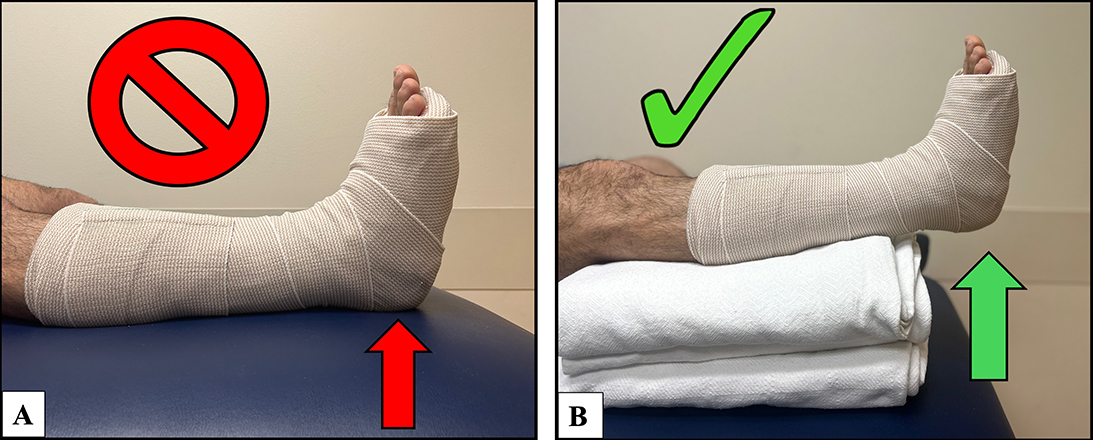
Figure 1: (A) A splint positioned while resting the heel down; the red arrow indicates the incorrect position of the heel. (B) A splint positioned while floating the heel freely; the green arrow indicates the correct position of the heel.
Courtesy of Erik R. Nakken, MD
Published 3/1/2026
A pressure transducer was placed over the posterior heel; this was used for all contact pressure measurements.
The first biomechanical study measuring contact pressure of the posterior heel to identify the optimal splint configuration and positioning for risk reduction of secondary injuries will be presented at the AAOS 2026 Annual Meeting.
Lower extremity plaster splints are widely used. However, splinting of the lower extremity poses a risk of posterior heel pressure injury, with 12% of medical device-related pressure injuries occurring after splinting or casting. Also, splint-induced skin ulceration has been reported as the second most common iatrogenic plastic surgery referral.
“After observing a couple of patients develop posterior heel pressure ulcers, we sought to identify which variables most effectively reduce posterior heel contact pressure within a splint,” said Erik R. Nakken, MD. “Specifically, we evaluated padding thickness, padding brand, and resting heel position. Although splint-related pressure injuries are uncommon and ideally represent a never event, we aimed to generate findings that could be readily translated into clinical practice to improve patient outcomes.”
The study used volunteer participants in a controlled setting at an academic medical center. Twenty legs in 10 healthy volunteer adults without current foot or ankle pathology were recruited for the study. A pressure transducer (Figure 1) was used over the posterior heel to measure peak contact pressure in a short leg splint. Peak contact pressures were measured with zero, two, four, six, eight, and 10 layers of two undercast padding brands, with the heel resting down on the treatment surface and with the heel floating freely (Figure 2). Pressures were compared to a 32 mmHg threshold (the pressure of dermal arteriolar capillary collapse).
“We were surprised to find that eight to 10 layers of padding posterior to the heel were required to reduce contact pressure below the threshold of dermal arteriolar capillary collapse (32 mmHg),” Dr. Nakken said. “Importantly, this reduction was only achieved when combined with floating the heel — positioning the lower extremity with support under the calf so the heel is completely offloaded.”
Adjusting for heel position and padding layers, the mean contact pressure decreased 15 mmHg when using Specialist padding compared with Wytex padding. However, inappropriately bunched or folded padding under the heel increased contact pressure, overcoming the benefit of additional padding layers. Six abnormal pressure spikes occurred during pressure testing related to improperly bunched undercast padding, increasing the mean contact pressure by roughly three-fold compared with evenly applied padding.
The peak contact pressure of the posterior heel in various splint configurations based on heel position (heel floating freely vs. heel resting down), padding thickness (0, 2, 4, 6, 8, and 10 layers of padding), and padding brand. SI conversion factor: to convert pressure (mmHg) to pascals, multiple values by 133. n = number, SD = standard deviation, % = percentage, CI = confidence interval, NA = not applicable, red highlights = average contact pressure measurements at or below the critical 32 mmHg threshold, mmHg = millimeters of mercury, a = number of legs under 32 mmHg (the pressure of dermal arteriolar capillary collapse) with percentage of legs achieving that threshold.
This study has limitations. The authors acknowledge that testing in a clinical environment is needed to confirm decreased incidence of iatrogenic pressure injury. Additionally, the study measured contact pressures of the posterior heel at only one time point in volunteers without current foot or ankle injuries. Patients requiring a lower extremity splint may have swelling after an injury. Also, position changes from recumbent to standing, and deformation of cotton padding over time may occur. The authors predict these factors may increase contact pressure over time, and their findings may underestimate the true long-term contact pressure. Further, none of the study participants were classified as obese. However, the participant with the lowest BMI exhibited the highest initial contact pressures, aligning with a previous study.
“Heel floating emerged as the most influential variable in our study,” Dr. Nakken explained. “These findings are particularly meaningful because both padding thickness and heel position are modifiable risk factors. As providers, we can be deliberate about applying eight to 10 uniform layers of padding and proactive in counseling patients and their families on the importance of heel offloading at home. We have since incorporated these instructions, along with visual aids, into our discharge materials sent home with patients, and hope that these small, practical changes will translate into meaningful improvements in patient care.”
Paper 132 will be presented during Case Chats: Foot and Ankle II – Hindfoot at 2 to 3 p.m. on Monday in room 221.
Dr. Nakken’s coauthors of “Can Simple Changes in Splinting Technique Reduce Posterior Heel Contact Pressure?” are Kempland C. Walley, MD; Carol A. Janney, PhD; Davin C. Gong, MD; Vandan Patel, MD; David M. Walton, MD; Paul Talusan, MD, FAAOS; and James R. Holmes, MD, FAAOS.
Theresa Witham is managing editor for AAOS Now.